
51° DHS CONFERENCE
HAMBURG, NOVEMBER 14-16TH 2011
Treatment and Rehabilitation in ItalianAddiction Services
New strategies in psycostimulant consumption
Augusto Consoli
Director Department Addiction Treatment Service,
National Health Service, Turin, Italy
� Liebe Kollègen und Kollèginen,
Ich bedanke Ihnen, mich auf dieser sehrinteressanten kongress in Hamburg eingeladenzu haben.
Leider kann ich nicht auf ihre schöne Sprachesprechen.
Dann werde ich mein Referat auf Englishvorstellen.
A SHORT HISTORY OF ITALIAN
SERVICES
�Three principal phases
� First phase from the end of the 1970s to
the end of the 1980s.
� Second phase relates to the period from
1990 to 1998
� Third phase extends from 1999 to today.
FIRST PHASE
�Law n.685 of 1975 , the service were born
�Growing social alarm
� Impossible tasks
�Very little scientific and professional
involvement
� “Dilettantes in jeopardy”
SECOND PHASE
� The law n. 162 of 1990
� More human and material resources were
available
� “Duty” integration of public and private
services
� Reorganization of Health system
� Greater responsibility, management
knowledge and clarity of objectives in every
service
� The attempt to increase the quality of service
THIRD PHASE
�Diffusion of the unified concept ofpathological dependence, which tries toconnect various behavioral addictions in onefundamental, comprehensive and unifiedexplanation
� Increasing of researches (for exampleVedette, sample of 11.000 people) and othertrials
� In various Regions an Agreement Actbetween the State and the Regions has beenapplied, regarding the expansion of theactivities performed by the TherapeuticCommunity in the field of addict assistanceand rehabilitation

THIRD FASE
�During the year 2006 it emerged an
important modification in the prescriptive
norms on the addiction sector.
�This change, that professionals did not
want, was all of sudden and unexpectedly
included in a series of norms related to
the 2006 Winter Olympic Games held in
Turin, Italy (!)
THIRD FASE
� In 2008 a previosly proposed norm was
enforced and a set of professionals (health
practitioners, drivers, pilots, crane
operators, etc) has been strictly monitored
as far as drug and alcohol usage is
concerned
THIRD FASE
�Regarding resources, one can see that
there has been a gradual reduction in
personnel dedicated to addiction
prevention and treatment, and that
therefore, at present, the situation is
precarious in both public and private
sectors.
THIRD FASE
�Lukily enough in some Italian areas it
was possible to establish various social
workers in particular those working in
low threshold and harm reduction services
THIRD FASE
� Today we encounter the following situationand several working subjects
� In 2010
� 550 Addiction Services
� More than 650 Therapeutic Communities
� Users on treatment have been about 200.000
� 56 out of 10000 inhabitants between 15 and54 years old
� A good connection with Pratictioners, SocialService, Court, Emergency Services, etc
SOME CRITICAL POINTS
�Many aspects concerning the quality
levels of services must be improved or
evenly spread around all the Italian
services.
�As far as the positive aspects are
concerned we may point out these four: 3
related to organization and 1 to socio-
cultural patterns
ORGANIZATION
1. The strong cooperation between pubblic
and private sectors represents a high
quality resource suitable to respond to
the complexity of patients’s issues

ORGANIZATION
2. -A widespread diffusion of surgeries and
clinics in every contest such as bigger and
smaller towns, mountain areas, holiday
resort etc) to ease up users’ access
-The constant availability of operators of
6 professional profiles to assure a
multiprofessional response
ORGANIZATION
3 -The effort to manage prevention areas,early diagnosis, treatment, rehabilitation,social inclusion and harm reduction bypreserving a specific and unique identityin the services.
-This should be implemented by opposingthe very high pressures to get fragmentedand absorbed into Psychiatric or otherlocal services
-This is considered as a very importantvalue to keep attentivness, sensitivity,application and quality in this field
SOCIAL-CULTURAL ASPECT
� The existence of a ‘Wet culture’ in alcoholconsumption, known as Mediterranean drinkingstyle, is convivial and moderat, with the firstcontacts with alcohol dating back to preadolescence,as opposed to a Northern Europen ‘Dry culture’
� Nowadays in Italy, in spite of an increase of bingedrinking, the ‘Wet culture’ ends up beeing aprotective factor both from a great deal of bingedrinking and from progression to alcohol addiction
� See, for example, the recent research comparingalcohol addiction, binge, and dinking style inFinland and Italy
QUESTIONS
�We know it is possible to share ideas onorganizational subjects
�But, is it possible to share cultural andancient habits by a people? and how?
� Is it possible to extent the moderatealcohol consumption as protective factorfor other drug use, for example forpsycostimulant consumption?
PSYCOSTIMULANT USE AND TREATMENT
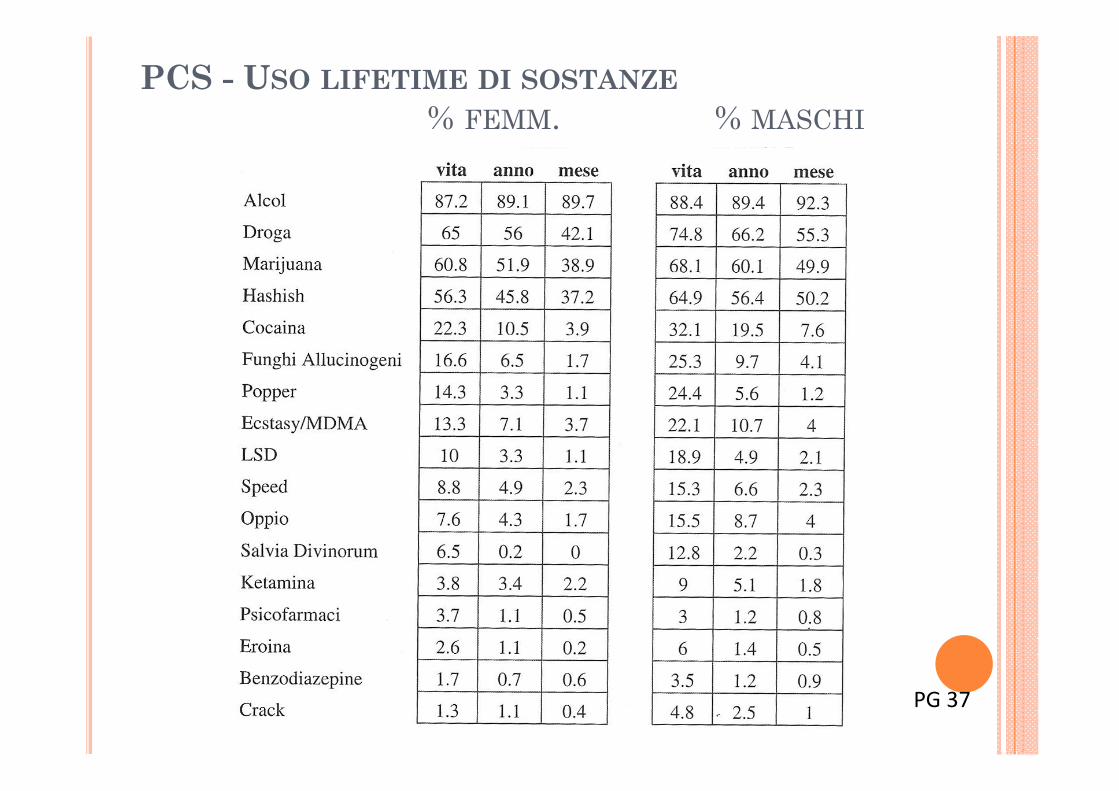
PCS - USO LIFETIME DI SOSTANZE
% FEMM. % MASCHI
PG 37

PG 47
ASSUMPTIONS_1
� The transversality of cocaine consumptions doesn’t
allow to identify a single intervention model for a very
heterogeneous typology of consumers, who need
different approaches and progressive objectives.
� We should deepen the reflection on the most suitable
procedures for receiving and taking charge of the
demands of people who often keep their own social and
affective dimensions separate from consumptions
hardly perceived as problematic.
ASSUMPTIONS_2
This perspective, which involves a redefinition of
traditional processes of access to the health care
services and which is oriented to promote the
emergence of hidden problems, invests both the
outpatient services as well as the residential ones
and the organizational structures as well as the
therapeutic settings.
MAIN QUESTION
Which factors must be evaluated in order to
select a good treatment for problematic
cocaine users?
GENERAL FACTORS
Individual factors (a) and environmental factors (b)
a)biological, cognitive, behavioral aspects (including
consumption patterns)
b)familiar, working, social factors (incl. illicit drugs
availability)
Adequacy (c) and accessibility (d) of treatment
c)referring to both therapists and patients
d)physical and cultural factors

CONSUMPTION PATTERNS
Typologies Age Patterns of use
Starter 16-18Episodic use; in group with other drugs and/or
alcohol; snorted or smoked
Weekender 18-25Occasional use; in group, with other drugs and/or
alcohol; snorted or smoked
Pure 18-25Continuous use; alone/ small group; episodic use
of other drugs; preserved social functioning; snorted, smoked, injected
Polyuser 18-35Continuous use of different drugs (cocaine, heroine, benzodiazepine, alcohol); snorted, smoked, injected
Relapser > 35Ex heroin or alcohol user; several cocaine relapse; former tretment courses; snorted, smoked, injected
Senior > 30Continuous use; episodic use of other drugs;
preserved social functioning; snorted, smoked, injected
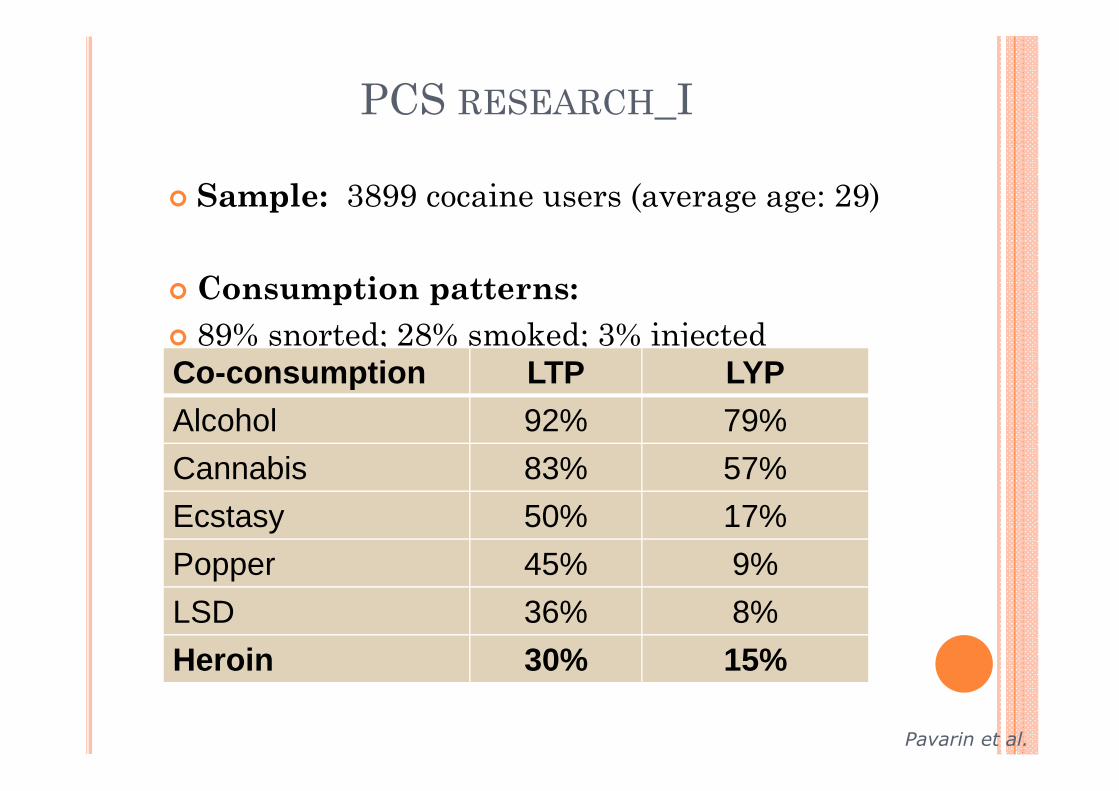
PCS RESEARCH_I
� Sample: 3899 cocaine users (average age: 29)
� Consumption patterns:
� 89% snorted; 28% smoked; 3% injected
Co-consumption LTP LYP
Alcohol 92% 79%
Cannabis 83% 57%
Ecstasy 50% 17%
Popper 45% 9%
LSD 36% 8%
Heroin 30% 15%
Pavarin et al.
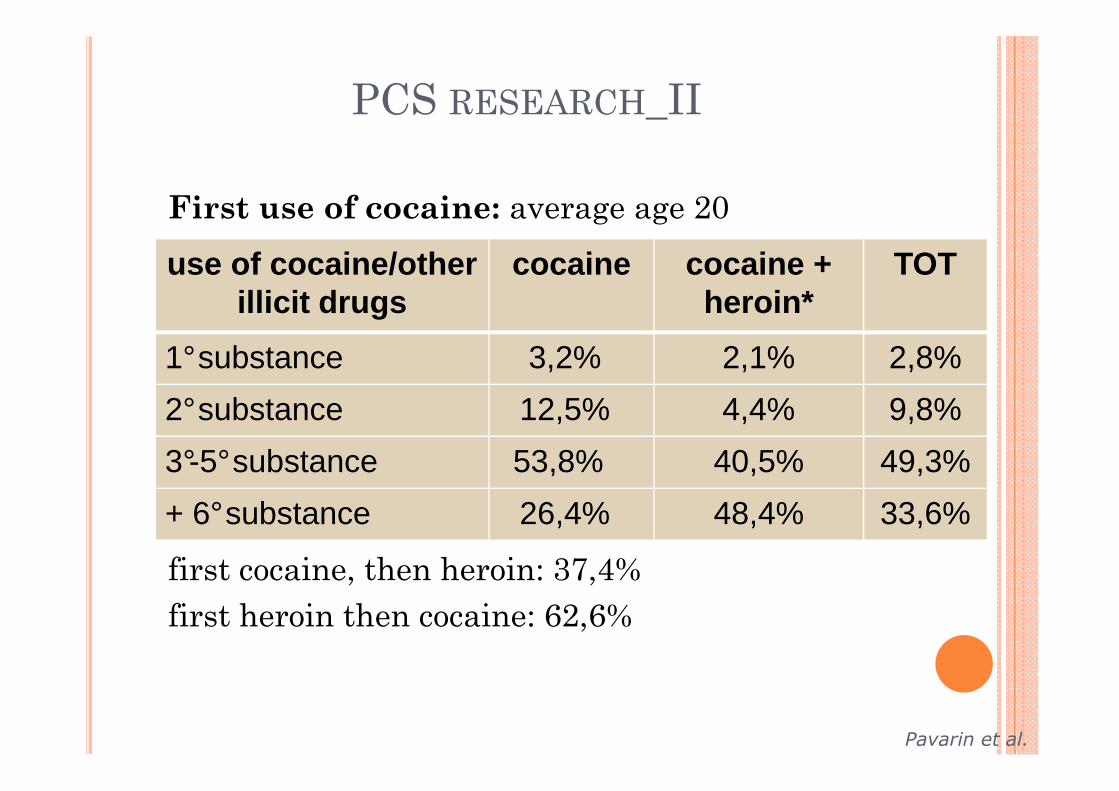
PCS RESEARCH_II
First use of cocaine: average age 20
*cocaine + heroin:
first cocaine, then heroin: 37,4%
first heroin then cocaine: 62,6%
use of cocaine/otherillicit drugs
cocaine cocaine + heroin*
TOT
1°substance 3,2% 2,1% 2,8%
2°substance 12,5% 4,4% 9,8%
3°-5°substance 53,8% 40,5% 49,3%
+ 6°substance 26,4% 48,4% 33,6%
Pavarin et al.
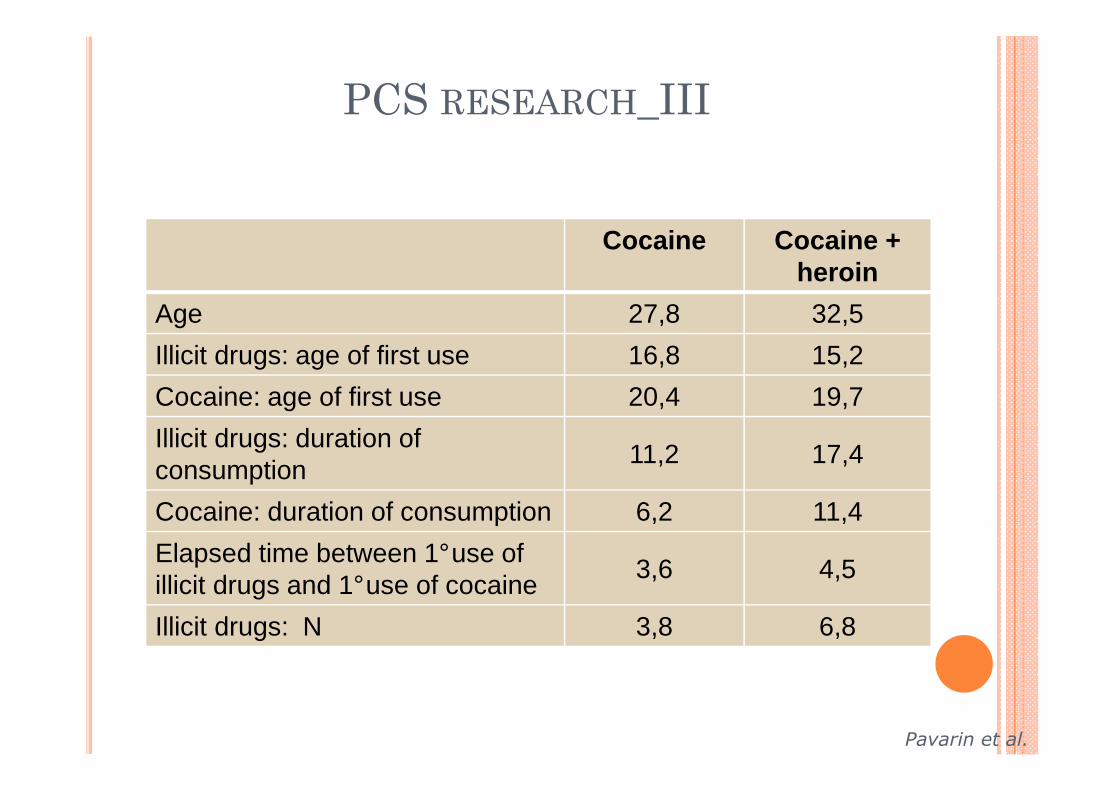
PCS RESEARCH_III
Cocaine Cocaine + heroin
Age 27,8 32,5
Illicit drugs: age of first use 16,8 15,2
Cocaine: age of first use 20,4 19,7
Illicit drugs: duration of consumption
11,2 17,4
Cocaine: duration of consumption 6,2 11,4
Elapsed time between 1°use of illicit drugs and 1°use of cocaine
3,6 4,5
Illicit drugs: N 3,8 6,8
Pavarin et al.
ITALIAN SITUATION ON COCAINE
TREATMENT
In Italy, over the last 7-8 years, several innovative
treatment projects have been developed to meet the
high spread of cocaine consumption, to which,
paradoxically, corresponds a limited care demand.
Many of these experiences has been monitored and
evaluated by National Cocaine Project, which
promoted collaboration between national/regional
and public/private structures.
NATIONAL COCAINE PROJECT - NCP
� The project , conceived for problemlatic cocaine users and
ATS, surveyed specialized treatment units. Such units were
created to respond to particular therapeutic user needs,
with the aim of enhacing and developing the treatment offer.
� Specifically, individual and group counseling, educational
intervention and psychotherapy (mainly CBT) have been
activated. The creation of these units was preceded by a
monitoring of specialized services already existing to assess
best practices and procedures. The project also included
widespread training activities in order to enhance specific
skills and general efficiency.
� The creation of these units was preceded by a
monitoring of specialized services already existing
to assess best practices and procedures. The
project also included widespread training activities
in order to enhance specific skills and general
efficiency
AIMS NCP
to highlight some features of different treatments and settings
to seek preliminary indications of possible auto-selection of
patients compared to different treatments and settings
to assess retention in treatment
compared to the profiles of treated patients
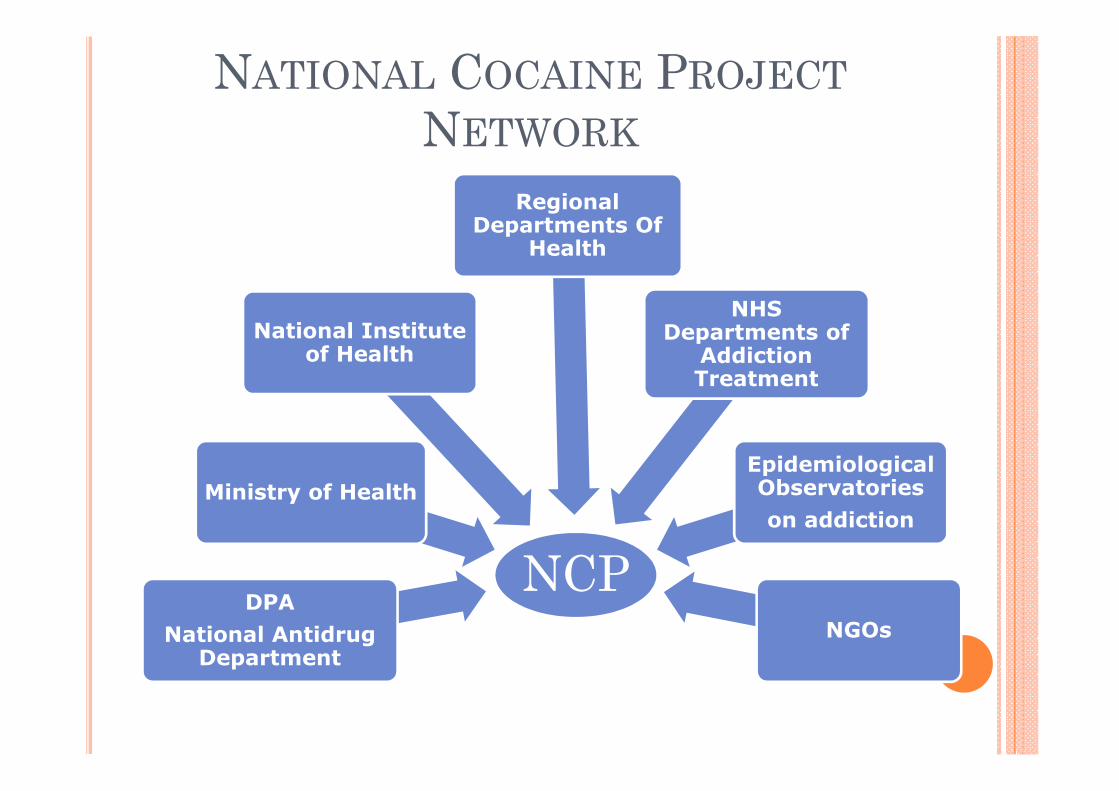
NATIONAL COCAINE PROJECT
NETWORK
NCPDPA
National AntidrugDepartment
Ministry of Health
National Instituteof Health
RegionalDepartments Of
Health
NHS Departments of
Addiction Treatment
EpidemiologicalObservatories
on addiction
NGOs
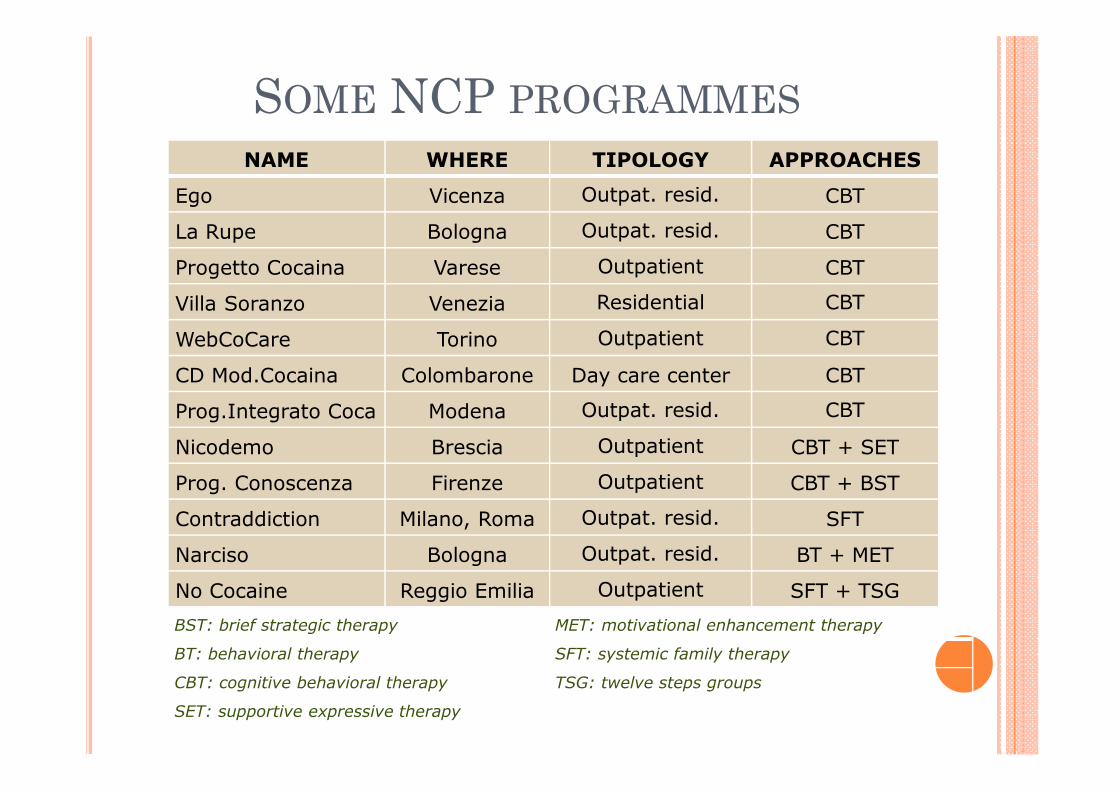
SOME NCP PROGRAMMES
NAME WHERE TIPOLOGY APPROACHES
Ego Vicenza Outpat. resid. CBT
La Rupe Bologna Outpat. resid. CBT
Progetto Cocaina Varese Outpatient CBT
Villa Soranzo Venezia Residential CBT
WebCoCare Torino Outpatient CBT
CD Mod.Cocaina Colombarone Day care center CBT
Prog.Integrato Coca Modena Outpat. resid. CBT
Nicodemo Brescia Outpatient CBT + SET
Prog. Conoscenza Firenze Outpatient CBT + BST
Contraddiction Milano, Roma Outpat. resid. SFT
Narciso Bologna Outpat. resid. BT + MET
No Cocaine Reggio Emilia Outpatient SFT + TSG
BST: brief strategic therapy MET: motivational enhancement therapy
BT: behavioral therapy SFT: systemic family therapy
CBT: cognitive behavioral therapy TSG: twelve steps groups
SET: supportive expressive therapy

SHARED AIMS
• to increase accessibility (web-based services, specialistic and non-traditional centers, extended opening hours/days,…);
• to offer more treatment options (parallel or sequential)consistent with the characteristics of the patients;
• to deepen the diagnostic evaluation (using standardizedinstruments also useful for clinical research) in the preliminarystages of the programme;
• to focus on motivation, through a brief but intense involvement;
• to encourage abstinence for the duration of the programme
• to allow patients to maintain their employment and activities.
1-COLOMBARONE COMMUNITY
CENTER� Target:
• Cocaine Users
• For ages 25-50
• No abstinence in outpatient program
• Frequent/severe relapses
� Programme duration:
• 2 preliminary counseling sessions
• 2 weeks + 2 days (total 10/12 consecutive days; Mon/Fri - h.9/17)
• for 3 months after the course: 12 group meetings once aweek
• 2 modules per year

COLOMBARONE COMMUNITY
CENTER
� Programme:
� Groups (10 people max)
• cognitive-behavioral
• craving management
• psycho-educational
• focal (here-and-now)
• learning and relaxation techniques
2-LA RUPE SHORT RESIDENTIAL
PROGRAM� Target:
• Cocaine users
• No psychiatric disorders
� Program duration:
• Time-out week-end
• Time-out 15 days
• Time-out 2 months

LA RUPE SHORT RESIDENTIAL
PROGRAM
� Program:
• intensive residential program (followed by
outpatient program);
• cognitive behavioral groups (max 10 pp.);
• individual counseling
• body-expression techniques.
3-WEBCOCARE WEBSITE
COUNSELING� Target:
• Cocaine users
• No exclusion criteria
� Program duration:
• preliminary web-based counseling (1 month)
• CBT (6 months)

Sostanze associate all'uso di cocaina
4,7% 5,3%
52,9%
5,9%
10,5%
46%
3,7%
0
10
20
30
40
50
60
Tipi di sostanze
Per
cent
uali
eroina
benzodiazepine
alcool
amfetamine
extasy
thc
lsd
Substances associated with cocaine use
alc
oh
ol
AT
S
ecsta
sy
TH
C
LS
D
BZ
D
he
roin
e%
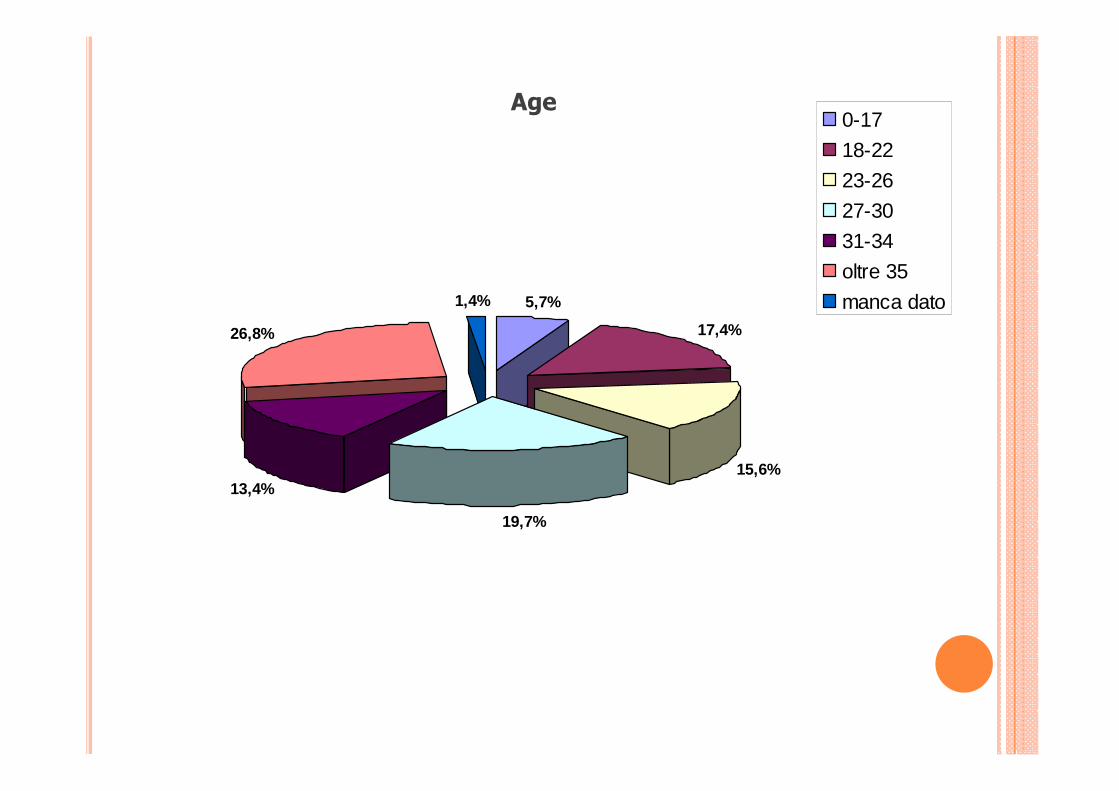
Età del campione
13,4%
19,7%
15,6%
17,4%
5,7%1,4%
26,8%
0-17
18-22
23-26
27-30
31-34
oltre 35
manca dato
Age

WEBCOCARE – ASI
Concluded (17) Interrupted (27) Comparison
MEAN SD MEAN SD T Test p
Medical 0,47 0,72 0,33 0,55 0,71 0,479
Employment 0,53 0,51 0,70 0,99 0,67 0,508
Alcohol 1,35 0,93 1,26 0,81 0,35 0,726
Drugs 2,53 0,51 2,81 0,68 1,48 0,146
Legal 0,18 0,39 0,22 0,51 0,31 0,752
Familiar 1,76 0,66 2,30 0,87 2,15 0,037
Psychological 1,88 0,70 2,37 0,69 2,28 0,027
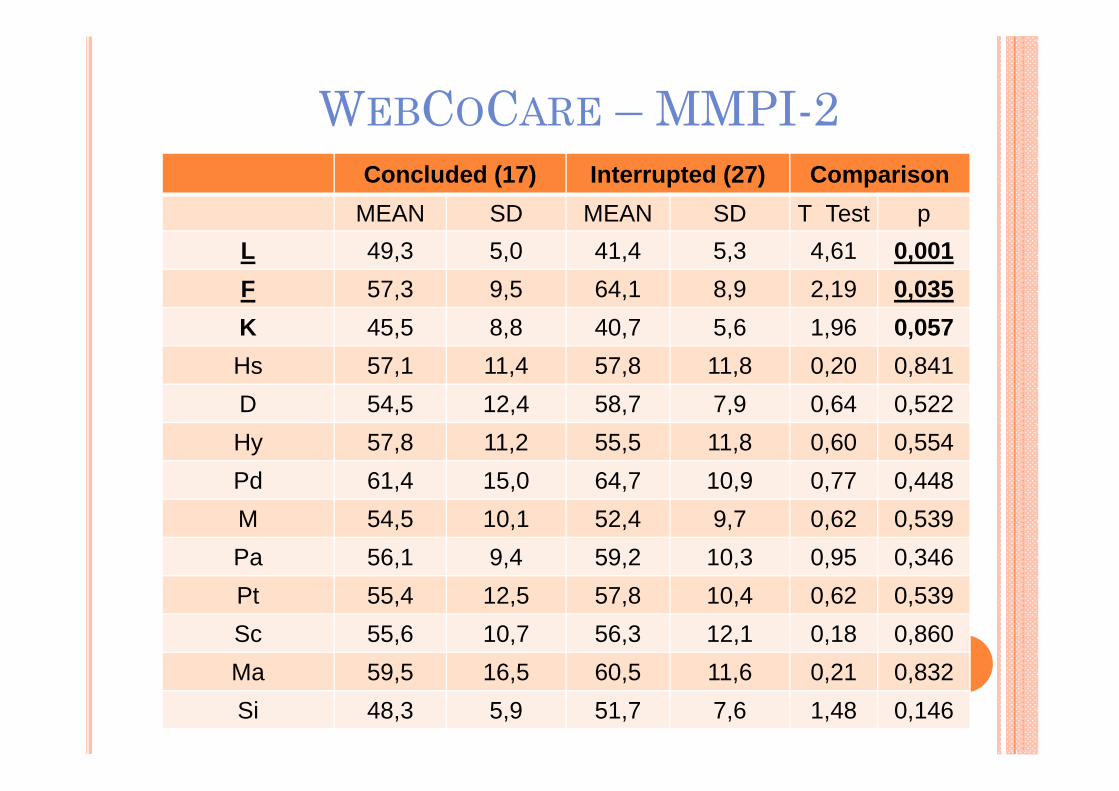
WEBCOCARE – MMPI-2
Concluded (17) Interrupted (27) Comparison
MEAN SD MEAN SD T Test p
L 49,3 5,0 41,4 5,3 4,61 0,001
F 57,3 9,5 64,1 8,9 2,19 0,035
K 45,5 8,8 40,7 5,6 1,96 0,057
Hs 57,1 11,4 57,8 11,8 0,20 0,841
D 54,5 12,4 58,7 7,9 0,64 0,522
Hy 57,8 11,2 55,5 11,8 0,60 0,554
Pd 61,4 15,0 64,7 10,9 0,77 0,448
M 54,5 10,1 52,4 9,7 0,62 0,539
Pa 56,1 9,4 59,2 10,3 0,95 0,346
Pt 55,4 12,5 57,8 10,4 0,62 0,539
Sc 55,6 10,7 56,3 12,1 0,18 0,860
Ma 59,5 16,5 60,5 11,6 0,21 0,832
Si 48,3 5,9 51,7 7,6 1,48 0,146
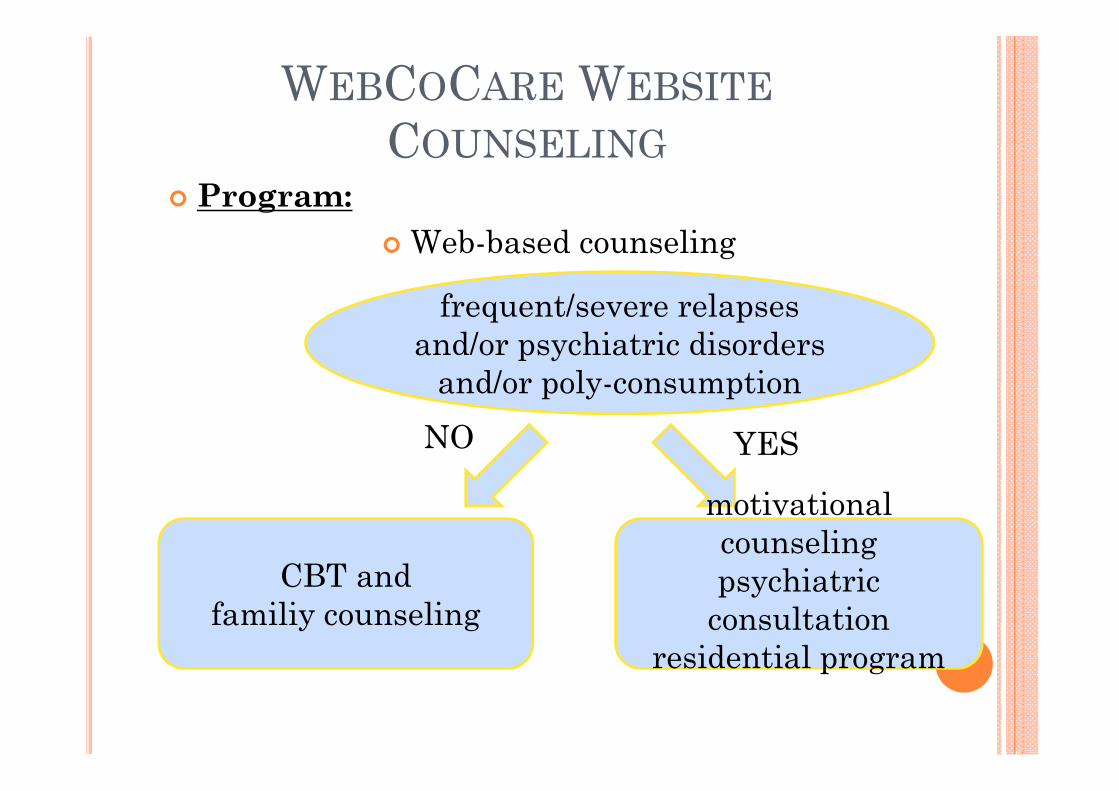
WEBCOCARE WEBSITE
COUNSELING
� Program:
� Web-based counseling
frequent/severe relapses
and/or psychiatric disorders
and/or poly-consumption
NO YES
CBT and
familiy counseling
motivational
counseling
psychiatric
consultation
residential program
CONCLUSIONS
• For cocaine treatment we need a redefinition oftraditional processes of access to the healthcare services and which is oriented to promotethe emergence of hidden problems.
• About clinical perspective our work shows
that:
a) some areas of functioning of the person
seem to be predictive of retention in CBT,
as well as some self-perceptions and
attitudes towards therapy;
b) the personality traits do not seem related
to retention.
CONCLUSIONS
• Other research should be focused on
selecting the most appropriate treatment
for cocaine users:
o identifying shared indicators of
effectivness;
o seeking further predictive indicators of
effectivness by studying:
• patients characteristics (symptoms,
autonomy, craving, ...)
• treatments characteristics (contexts, duration,
therapists, ...)
CONCLUSIONS
Actually we know that some treatments (CBT,
community reinforcement, contingency
management) shows a good effectiveness in
treating cocaine users, but we have to better
investigate the relationship between type of
patients and type of treatments.
Danke schön für Ihre
Aufmerksamkeit







