
Notärztliche Versorgung beim ACS
Univ.-Prof. Dr. Martin Möckel, FESC, FAHA
Dept. of Cardiology, Division of Emergency Medicine
Forum Herz
• Fallvignette I
• Präklinische Therapie beim STEMI
• (Diagnostische) Qualität der Notarztversorgung
• Fallvignette II
• (Prä)klinische Therapie beim NSTEMI
• Zusammenfassung und Schlussfolgerungen
Agenda
54 Jahre, männlich
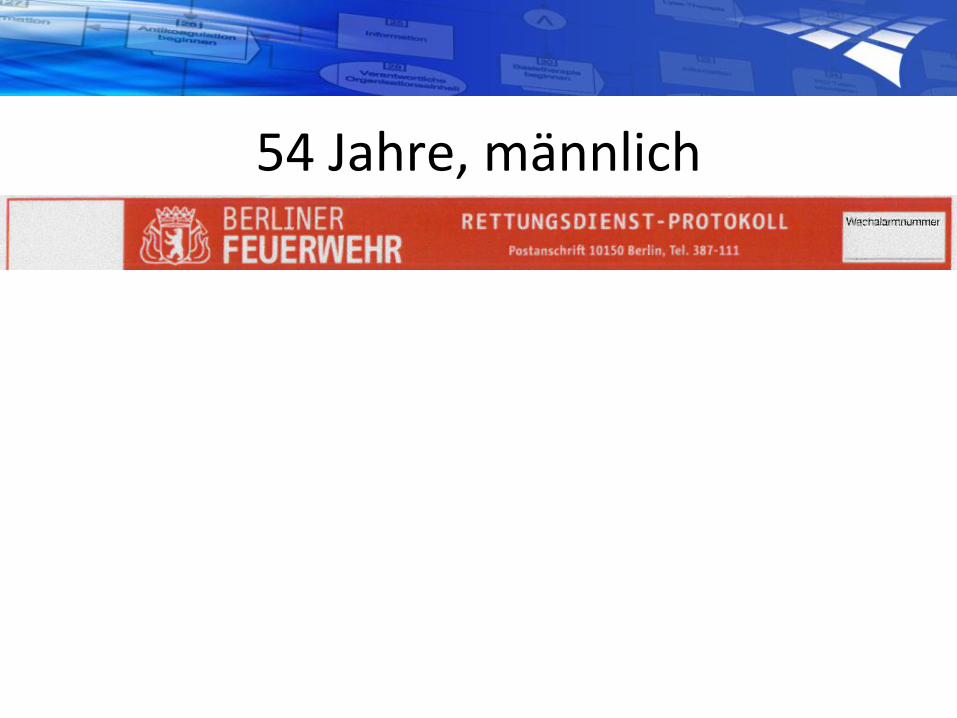
Rettungsdienst - Notarztwagen
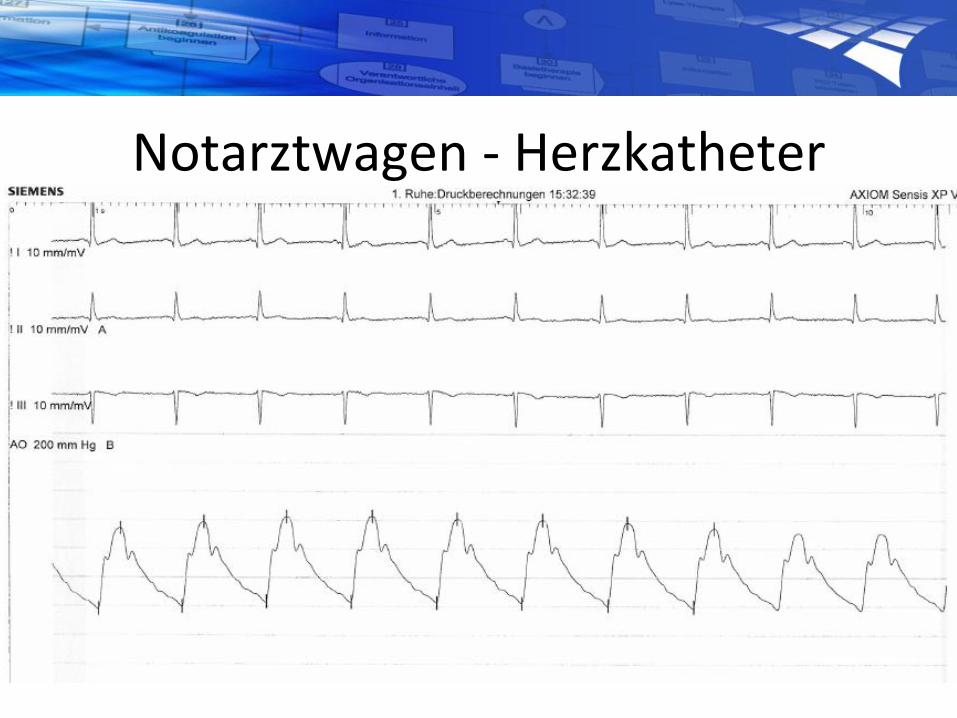
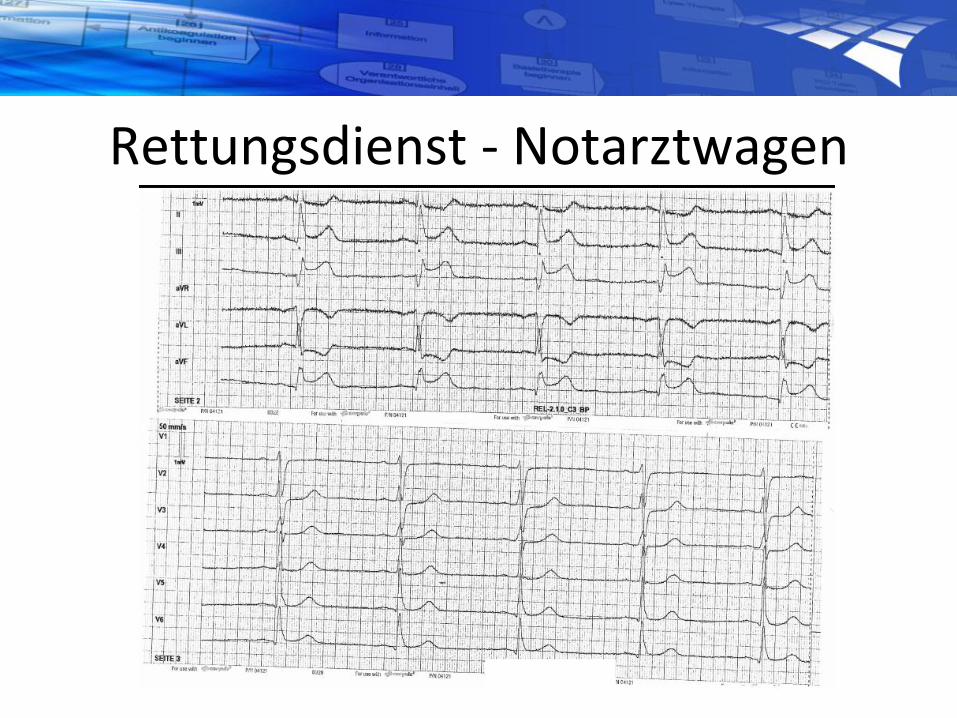
Notarztwagen - Herzkatheter


Klinik - Rehabilitation

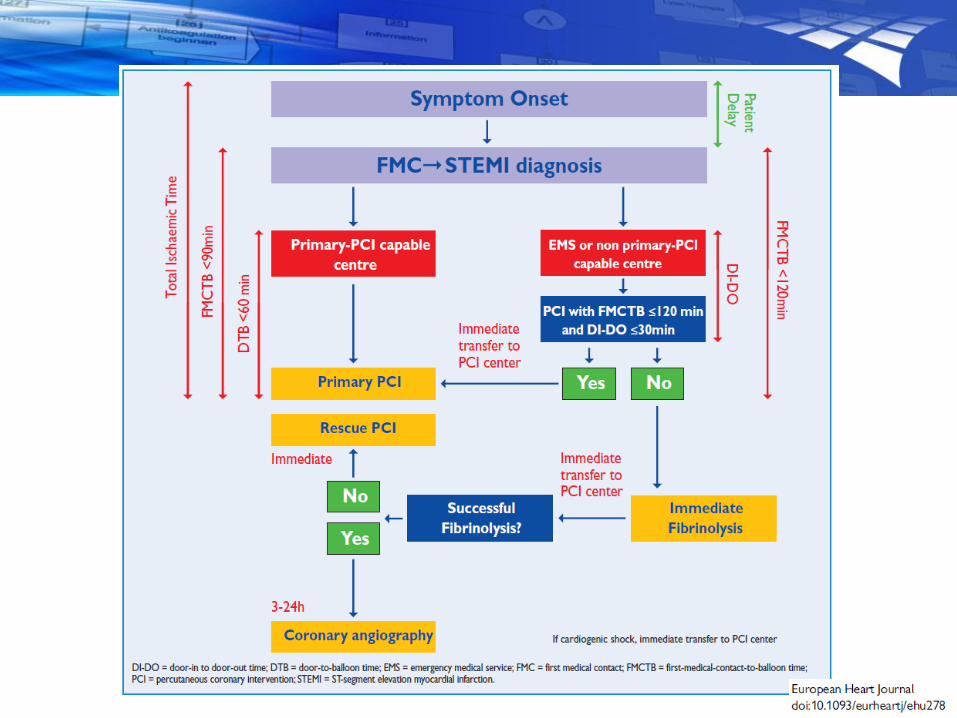
Empfehlungen beim STEMI

ATLANTIC
Eine Studie zum „Preloading“ beim STEMI
• Ticagrelor reduziert kardiovaskuläre Todesfälle, Herzinfarkte und Schlaganfälle im Vergleich zu Clopidogrel beim ACS in der PLATO-Studie[Wallentin 2009]; die Subgruppe der STEMI-Patienten profitiert ebenfalls[Steg 2010]
• Bislang gab es keine Studien, die explizit die prähospitale Gabe von Ticagrelor randomisiert untersucht haben[Montalescot 2013]
• Primäres Studienziel war daher die Bestimmung des optimalen Timings der Medikation mit Ticagrelor bei Patienten mit STEMI vor PCI
• Zusätzliche Substudie zur Thrombozytenhemmung
• Montalescot G et al. Am Heart J 2013;165:515–522; Steg PG et al. Circulation 2010;122:2131–2141;Wallentin L et al. N Engl J Med 2009;361:1045–1057
Ticagrelor
180 mg loading dose
Placebo
loading dosePre-hospital
Placebo
loading dose
Ticagrelor
180 mg loading doseIn-hospital
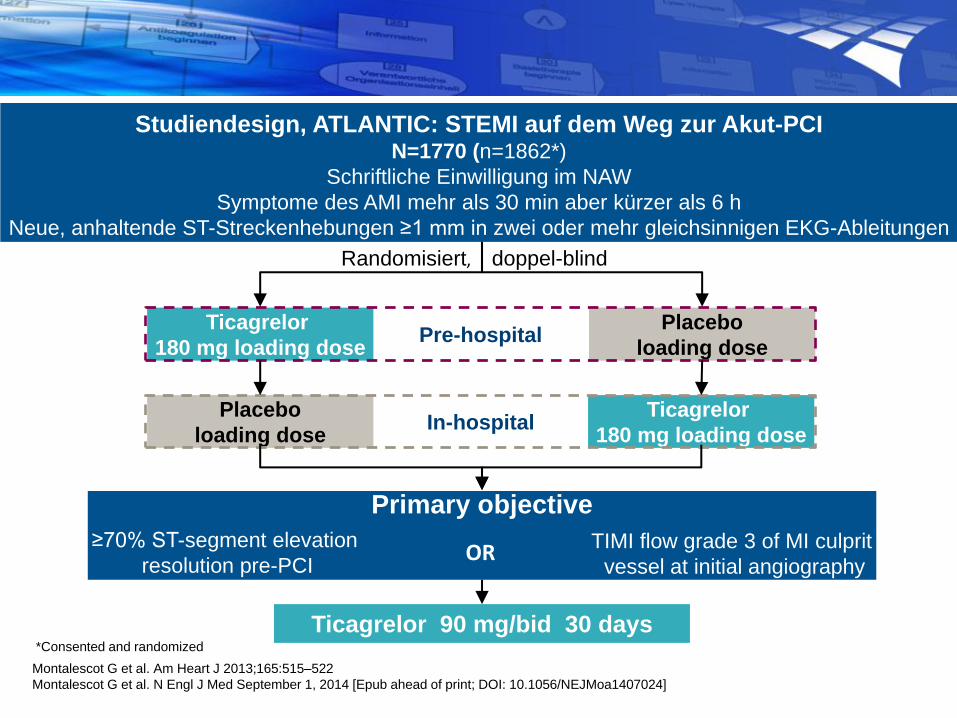
Randomisiert, doppel-blind
Ticagrelor 90 mg/bid 30 days
Primary objective
OR
Studiendesign, ATLANTIC: STEMI auf dem Weg zur Akut-PCIN=1770 (n=1862*)
Schriftliche Einwilligung im NAW
Symptome des AMI mehr als 30 min aber kürzer als 6 h
Neue, anhaltende ST-Streckenhebungen ≥1 mm in zwei oder mehr gleichsinnigen EKG-Ableitungen
≥70% ST-segment elevation
resolution pre-PCITIMI flow grade 3 of MI culprit
vessel at initial angiography
*Consented and randomized
Montalescot G et al. Am Heart J 2013;165:515–522
Montalescot G et al. N Engl J Med September 1, 2014 [Epub ahead of print; DOI: 10.1056/NEJMoa1407024]
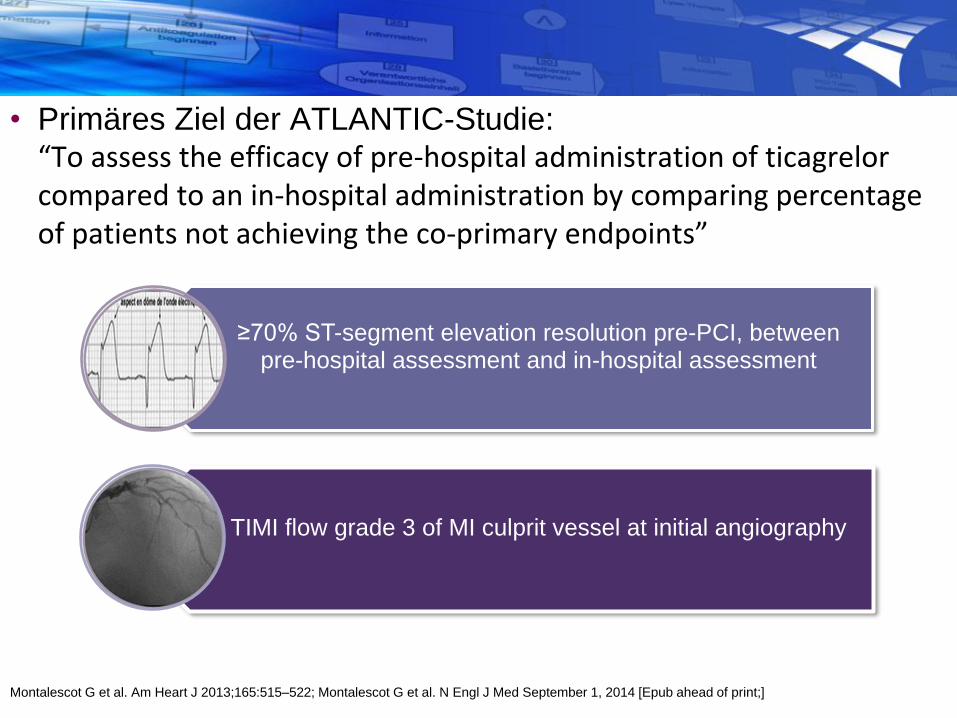
• Primäres Ziel der ATLANTIC-Studie:“To assess the efficacy of pre-hospital administration of ticagrelor compared to an in-hospital administration by comparing percentage of patients not achieving the co-primary endpoints”
≥70% ST-segment elevation resolution pre-PCI, between pre-hospital assessment and in-hospital assessment
TIMI flow grade 3 of MI culprit vessel at initial angiography
Montalescot G et al. Am Heart J 2013;165:515–522; Montalescot G et al. N Engl J Med September 1, 2014 [Epub ahead of print;]
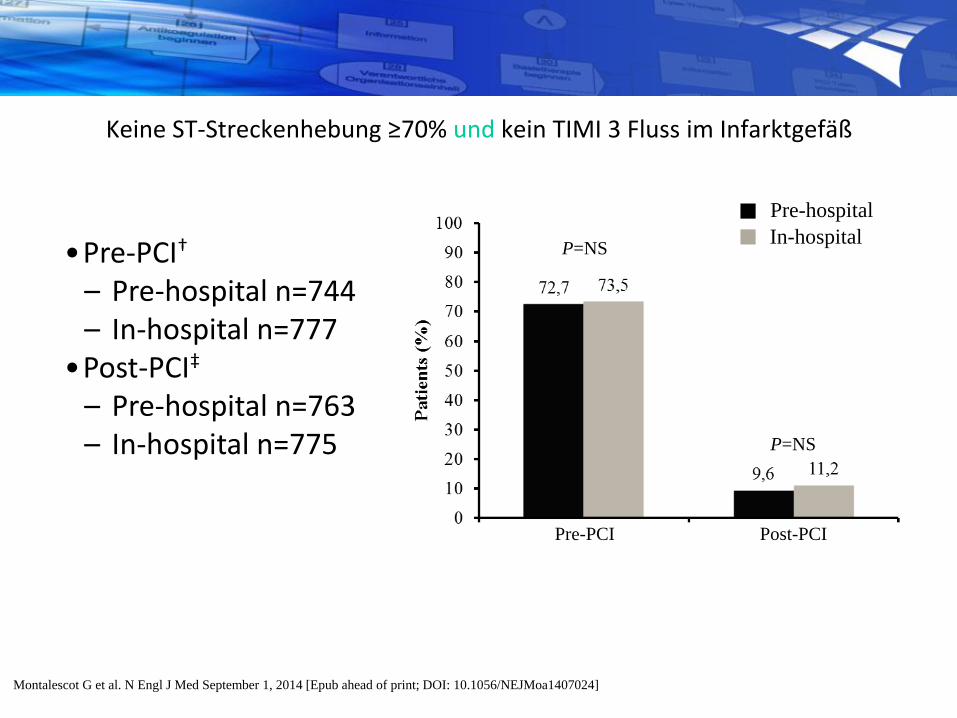
Keine ST-Streckenhebung ≥70% und kein TIMI 3 Fluss im Infarktgefäß
•Pre-PCI†
– Pre-hospital n=744– In-hospital n=777
•Post-PCI‡
– Pre-hospital n=763– In-hospital n=775
P=NS
P=NS
Pre-hospital
In-hospital
Pre-PCI Post-PCI
Montalescot G et al. N Engl J Med September 1, 2014 [Epub ahead of print; DOI: 10.1056/NEJMoa1407024]

Montalescot G et al. N Engl J Med September 1, 2014 [Epub ahead of print; DOI: 10.1056/NEJMoa1407024]

2
1
Definitive akute Stent Thrombose innerhalb von 30 Tagen
1
Ticagrelor pre-hospital 2/906 (0.2%) vs
ticagrelor in-hospital 11/952 (1.2%)
OR 0.19 (95% CI 0.04, 0.86), P=0.02
0 6 12 18 24 302 8 14 20 264 10 16 22 28
Ev
en
t ra
te (
KM
%)
0
Time (days)
Ticagrelor pre-hospitalTicagrelor in-hospital
24 h
P=0.008
30 days
P=0.02
Montalescot G et al. N Engl J Med September 1, 2014 [Epub ahead of print; DOI: 10.1056/NEJMoa1407024]

Prozeduren

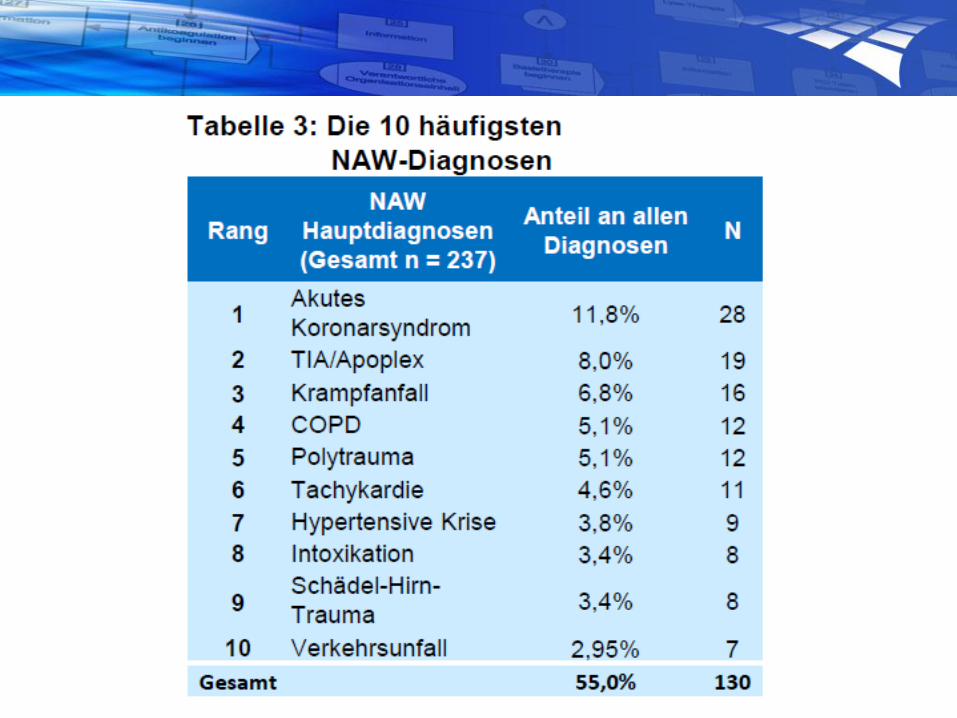
Wie gut ist die Diagnose des Notarztes?

Patient characteristics in
pre-hospital medical care
Johann Frick, Anna Slagman, Julia Searle, Clara Thomas, Judith Mahlig,
Tobias Lindner, Martin Möckel
Division of Emergency Medicine and Chest Pain Units (CVK, CCM),
Charité - Universitätsmedizin Berlin
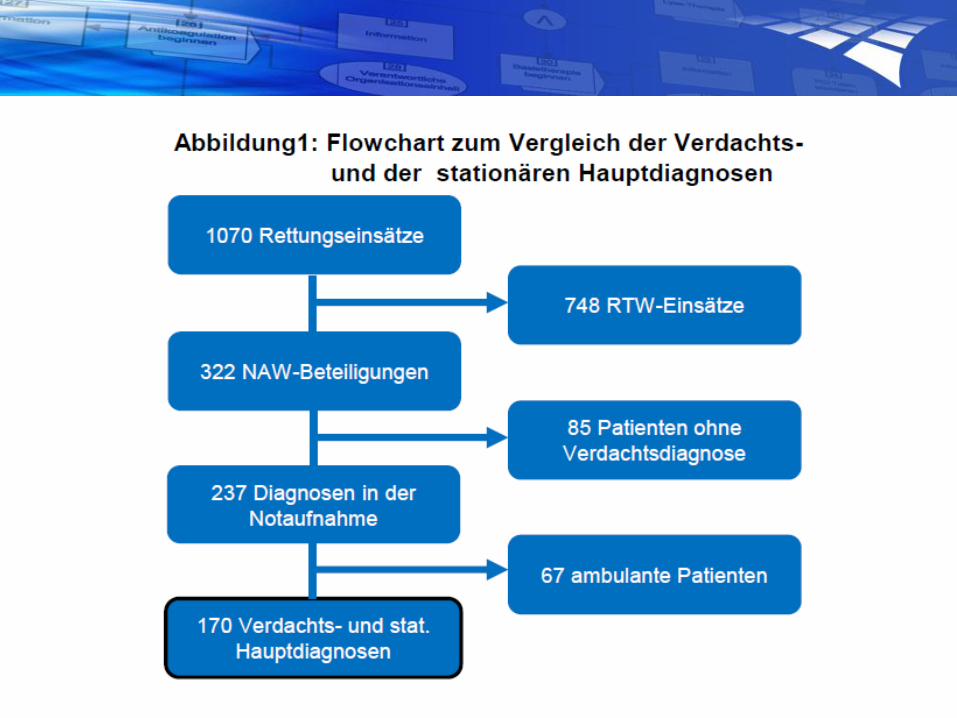
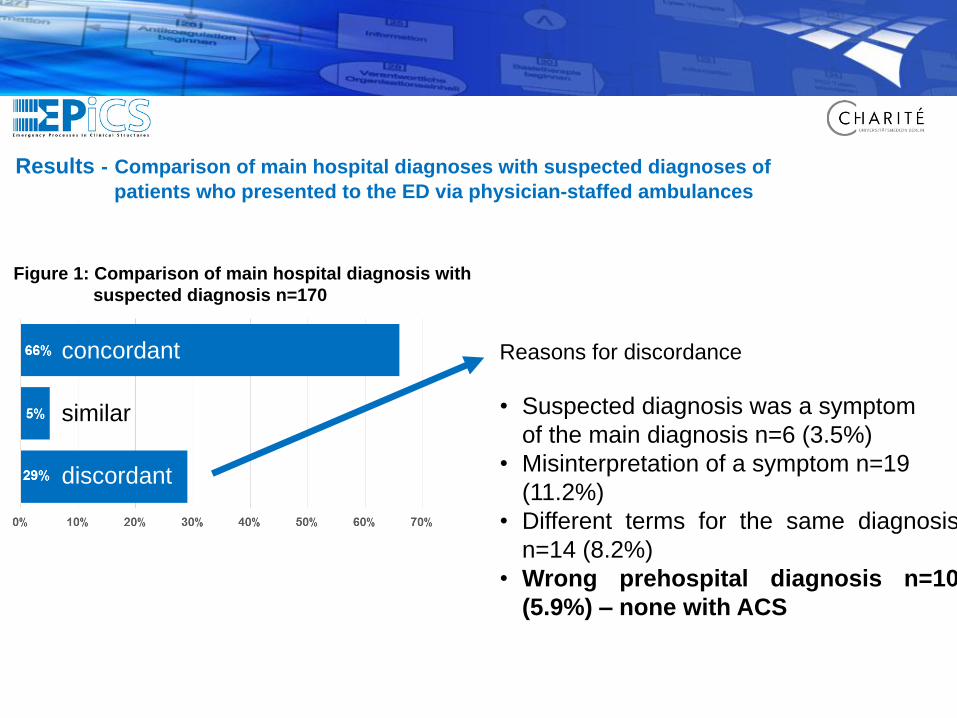
Results - Comparison of main hospital diagnoses with suspected diagnoses of
patients who presented to the ED via physician-staffed ambulances
Figure 1: Comparison of main hospital diagnosis with
suspected diagnosis n=170
Johann Frick, Anna Slagman, Julia Searle, Clara Thomas, Judith Mahlig, Tobias Lindner, Martin Möckel
Division of Emergency Medicine and Chest Pain Units(CVK, CCM), Charité - Universitätsmedizin Berlin
Reasons for discordance
• Suspected diagnosis was a symptom
of the main diagnosis n=6 (3.5%)
• Misinterpretation of a symptom n=19
(11.2%)
• Different terms for the same diagnosis
n=14 (8.2%)
• Wrong prehospital diagnosis n=10
(5.9%) – none with ACS
similar
discordant
concordant


44 Jahre, männlich• Seit mehreren Tagen rezidivierende AP
• Typ 1 Diabetes mellitus
• Chronische Niereninsuffizienz beiV.a. diabetische Nephropathie
• Aktuell Vorstellung in der Notaufnahme wegen Mischintoxikation in fraglich suizidaler Absicht mit Ibuprofen, Pipamperon (sedierendes Neuroleptikum), Viagra, Alkohol
• Vitalzeichen normal, Patient somnolent
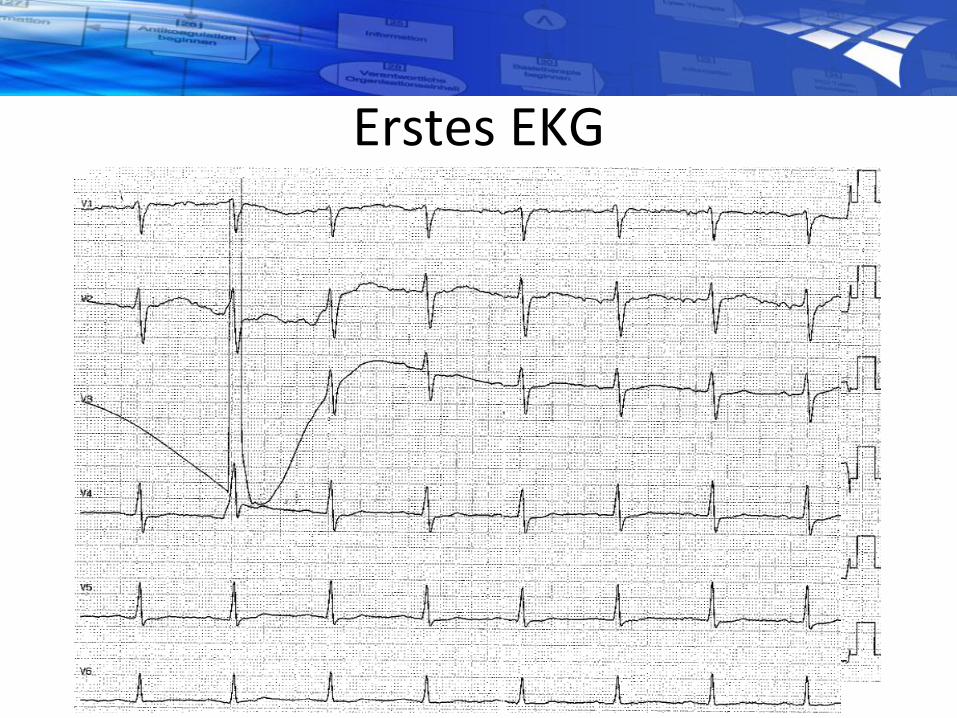
Erstes EKG
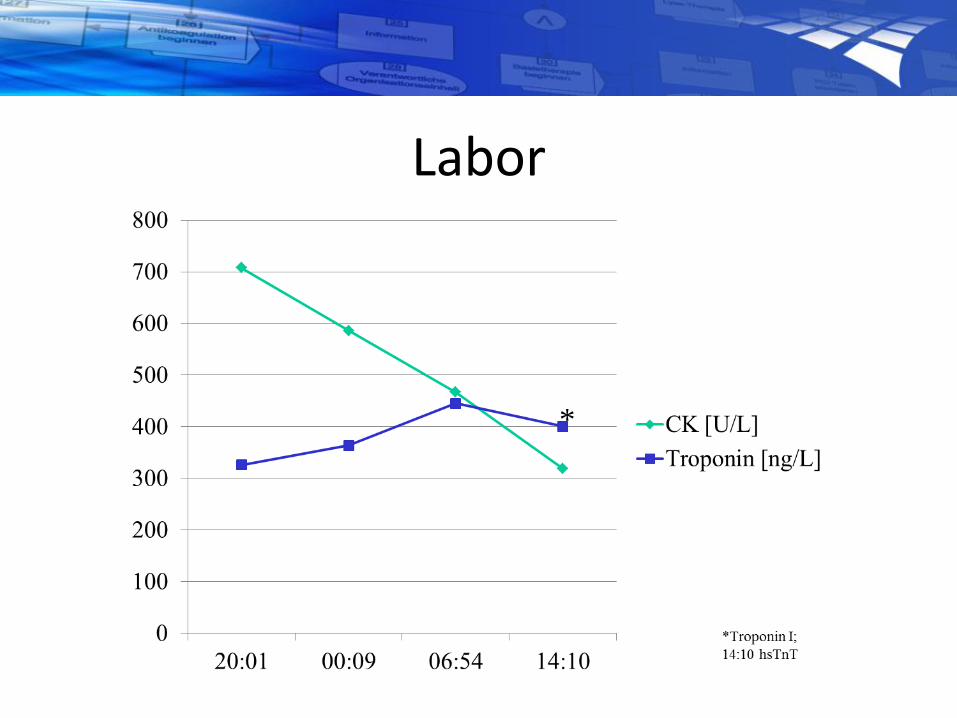
Labor
*
Verlauf (1)• Intensivüberwachung
• Patient kardiopulmonal stabil, keine AP mehr; Kreatinin 132µmol/L (1,5mg/dL)
• Kontaktaufnahme Charité: ASS, Heparin, Loading Ticagrelor 180mg; Verlegung zur invasiven Diagnostik sobald wie möglich
• Weitere Medikation: Insulinperfusor
• Verlegung am Folgetag geplant

Herzkatheter• Normale Pumpfunktion
• Schwere diffuse 3-Gefäß-KHK

Verlauf (2)• Herzteam: Entscheidung zur dringlichen OP am
Folgetag; Ticagrelor pausiert
• Intensivüberwachung, psychiatrisches Konsil:
• Erfolgreiche OP; aus dem Bericht:Bei guter Bluttrockenheit Sternumverschluß mit Drahtcerclagen.
• Unkomplizierter weiterer Verlauf; Rückverlegung zuweisendes Krankenhaus, stationäre ReHa
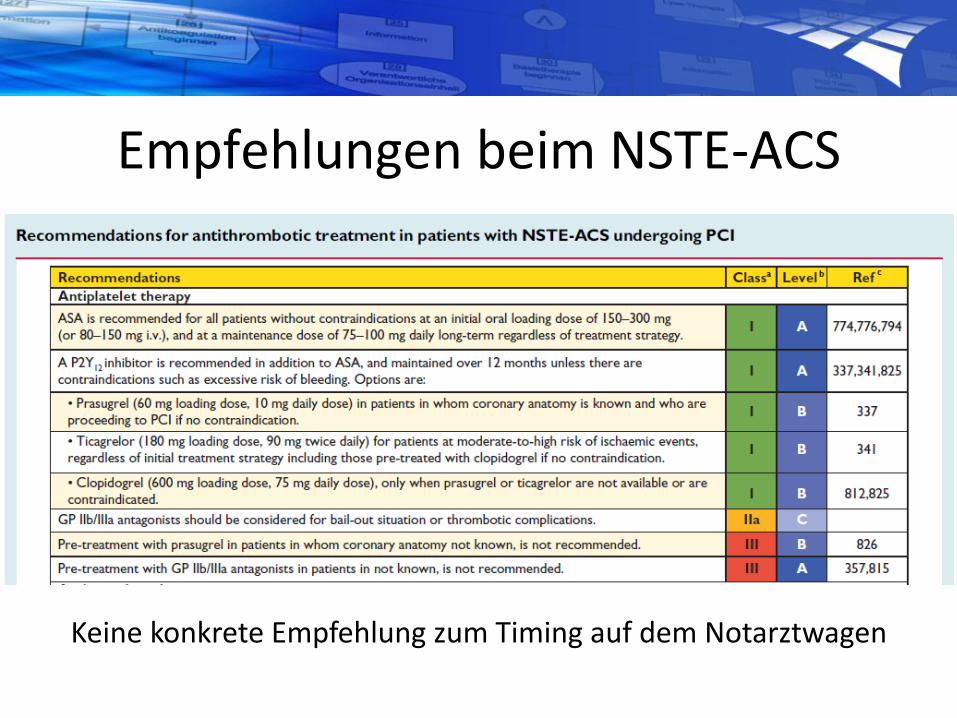
Empfehlungen beim NSTE-ACS
Keine konkrete Empfehlung zum Timing auf dem Notarztwagen

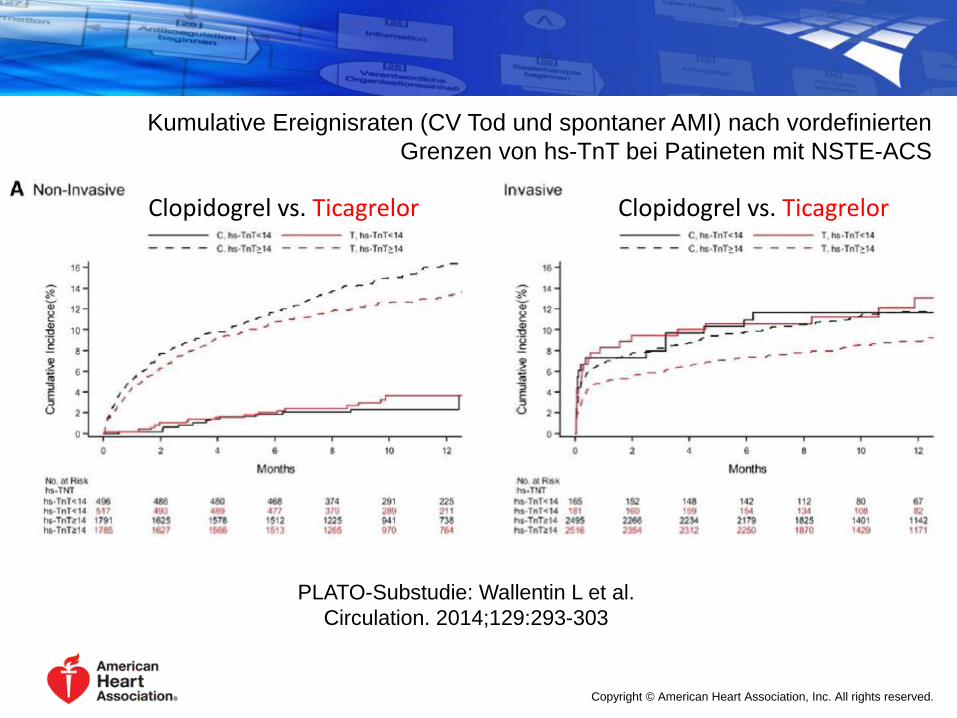
Kumulative Ereignisraten (CV Tod und spontaner AMI) nach vordefinierten
Grenzen von hs-TnT bei Patineten mit NSTE-ACS
PLATO-Substudie: Wallentin L et al.
Circulation. 2014;129:293-303
Clopidogrel vs. Ticagrelor Clopidogrel vs. Ticagrelor
Copyright © American Heart Association, Inc. All rights reserved.

PLATO-Substudie, Varenhorst et al. JACC 2012, 60:1623-30

Tod durch Blutung
Tod durch Infektion

• Das Notarztwesen in Deutschland ist gut etabliert und von hoher fachlicher und organisatorischer Qualität
• Die Erstversorgung des STEMI ist eine Domäne des Notarztes mit einem Focus auf dem schnellen und sicheren Transport
• Die präklinische Pharmakotherapie enthält heute häufig auch bereits einen zweiten Plättchenhemmer(Ticagrelor, Prasugrel)
• Für das Outcome des Patienten ist der intersektorale Behandlungspfad besonders bedeutsam

http://notfallmedizin.charite.de
1910







