Cardiac Surgery
University of Rostock
7. IGES Kongress zum Fortschritt im Gesundheitswesen von morgen
22. October 2009
Wiederherstellung der Herzfunktion durch Stammzelltherapie
Prof. Dr. med. Gustav Steinhoff
Director
Reference and Translation Center of Cardiac Stem Cell Therapy (RTC)
and
Department of Cardiac Surgery
University of Rostock
Cardiac Surgery
University of Rostock
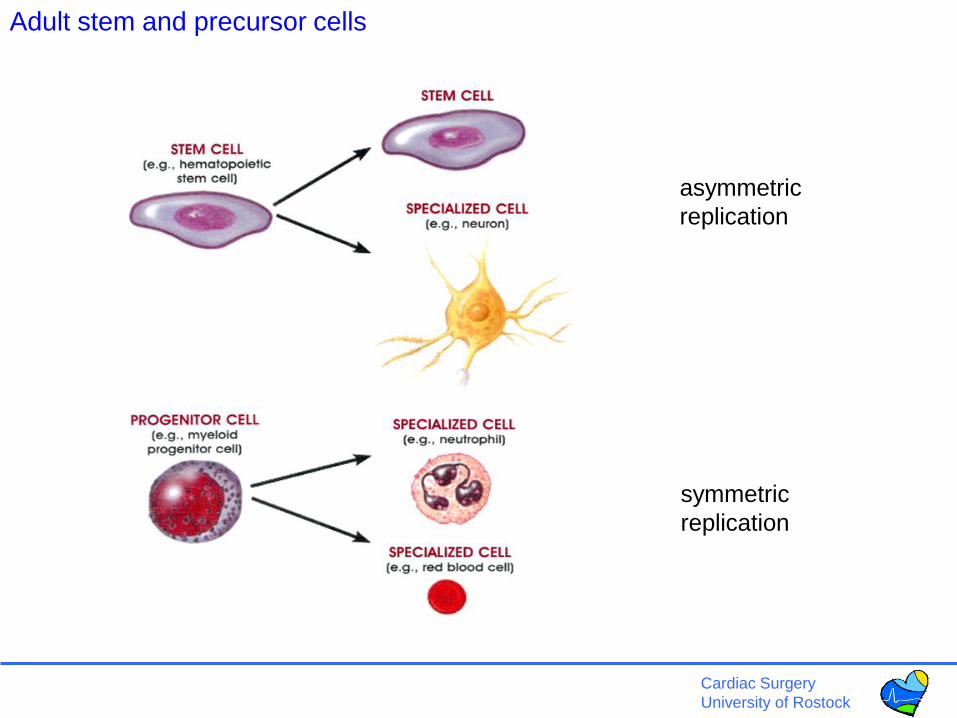
asymmetric
replication
symmetric
replication
Adult stem and precursor cells
Cardiac Surgery
University of Rostock
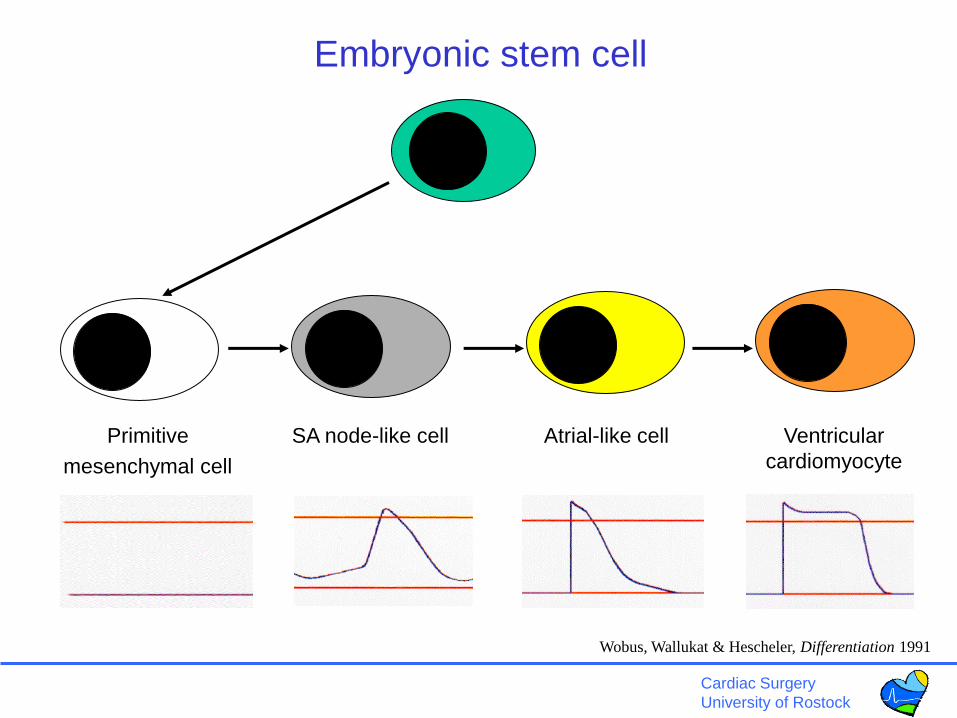
Embryonic stem cell
Wobus, Wallukat & Hescheler, Differentiation 1991
Primitive
mesenchymal cell
SA node-like cell Ventricular
cardiomyocyte
Atrial-like cell
Cardiac Surgery
University of Rostock
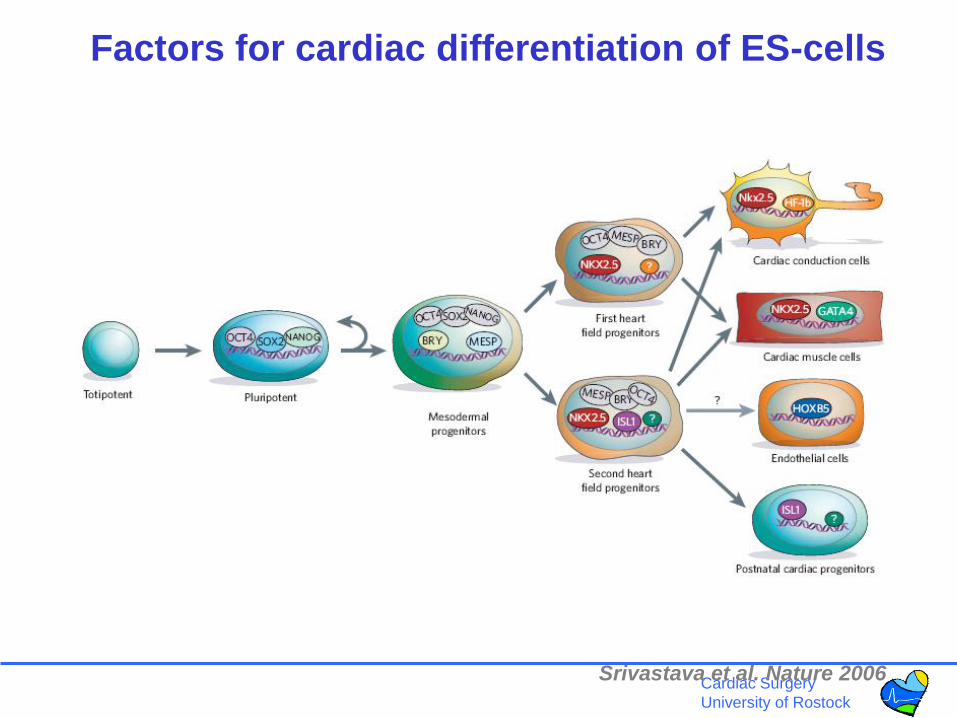
Factors for cardiac differentiation of ES-cells
Srivastava et al. Nature 2006
Cardiac Surgery
University of Rostock
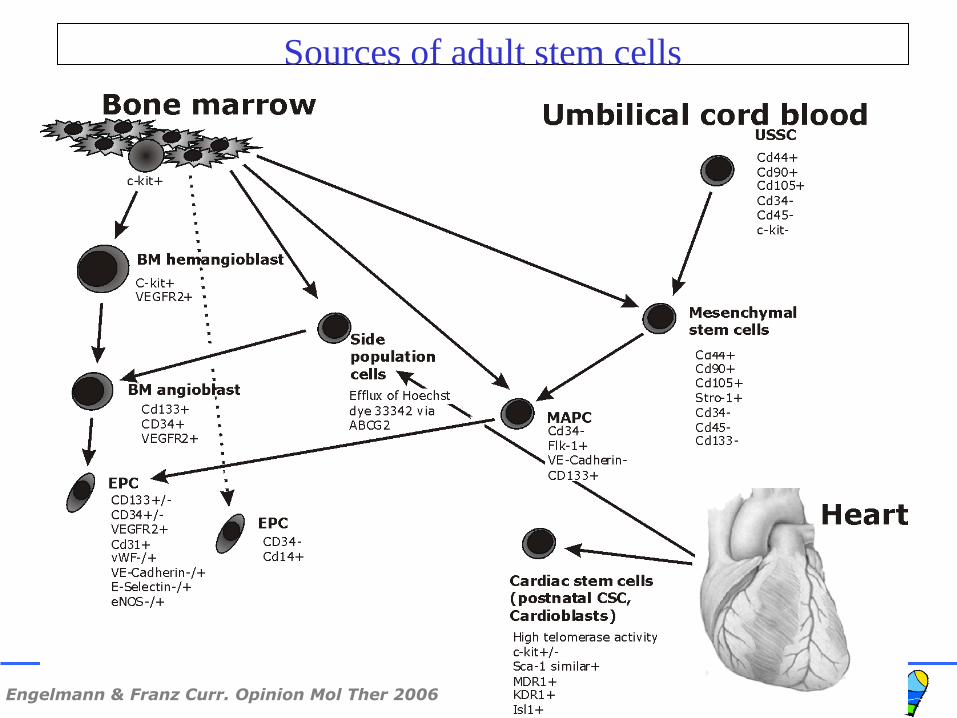
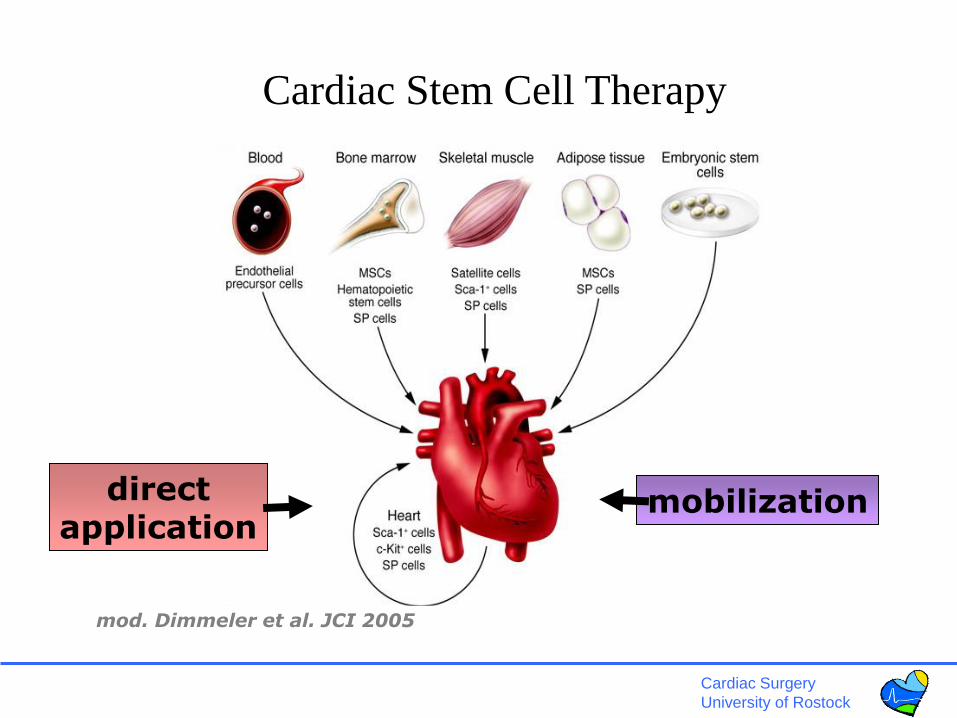
Sources of adult stem cells
Engelmann & Franz Curr. Opinion Mol Ther 2006

Cardiac Surgery
University of Rostock
Adult stem cells – bone marrow source
lifelong regeneration potential
Cardiac Surgery
University of Rostock
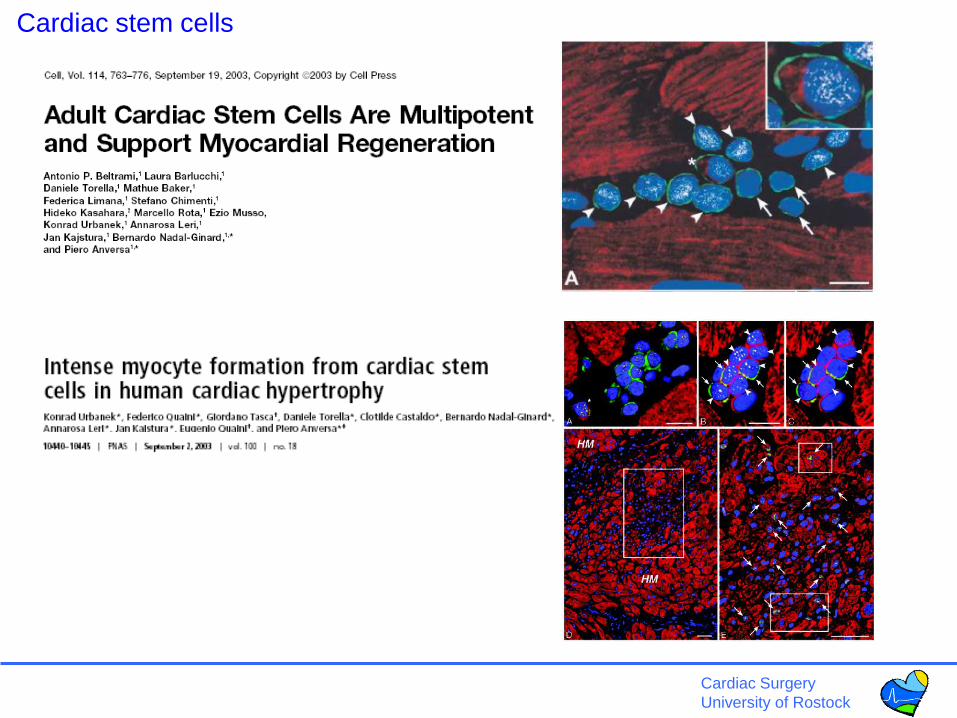
Cardiac stem cells
Cardiac Surgery
University of Rostock
The impact of stem cells in the future of cardiac therapies
• Stem cells in heart failure treatment
• Stem cells and bridge-to-recovery/ bridge-to-transplant
• Stem cells and immunomodulation after heart
transplantation
• Cellular chimerism and cellular renewal in heart
transplants
• Summary and outlook
Cardiac Surgery
University of Rostock
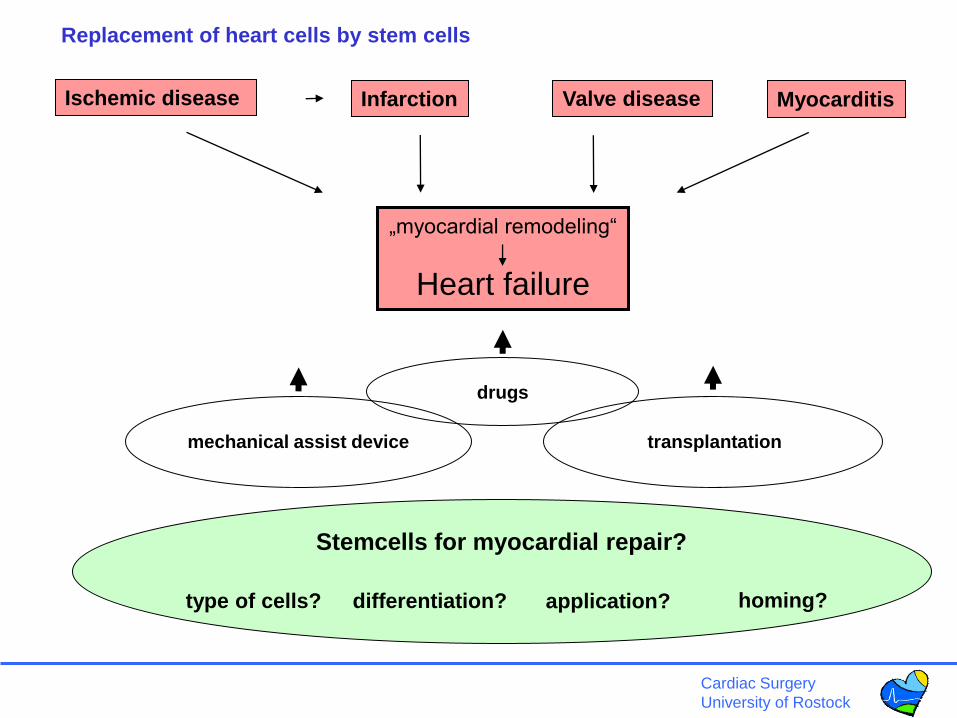
Ischemic disease Infarction
„myocardial remodeling“
Heart failure
Stemcells for myocardial repair?
application?type of cells? homing?
Valve disease Myocarditis
transplantationmechanical assist device
drugs
differentiation?
Replacement of heart cells by stem cells
Cardiac Surgery
University of Rostock
mod. Dimmeler et al. JCI 2005
directapplication
mobilization
Cardiac Stem Cell Therapy
Cardiac Surgery
University of Rostock
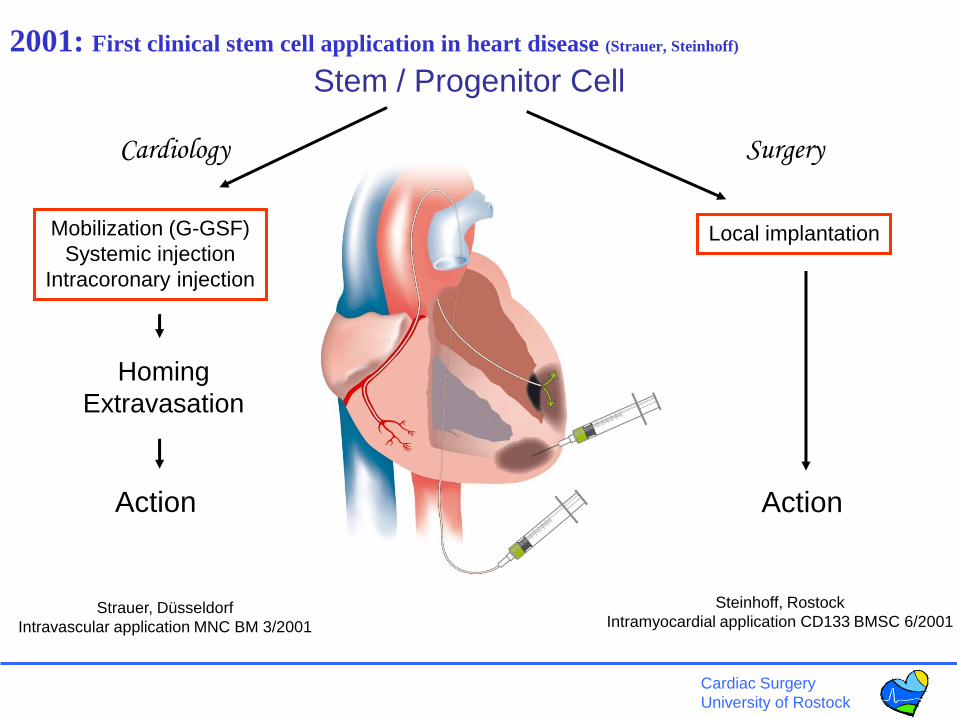
Cell delivery
Mobilization (G-GSF)
Systemic injection
Intracoronary injection
Local implantation
Action
Homing
Extravasation
Stem / Progenitor Cell
Action
SurgeryCardiology
Problems observed
2001: First clinical stem cell application in heart disease (Strauer, Steinhoff)
Strauer, Düsseldorf
Intravascular application MNC BM 3/2001
Steinhoff, Rostock
Intramyocardial application CD133 BMSC 6/2001

Cardiac Surgery
University of Rostock
Orlic D, Kajstura J, Chimenti S, Jakoniuk I, Anderson SM, Li B, et al. Bone marrow cells regenerate infarcted myocardium.
Nature. 2001 Apr 5;410(6829):701-5.
[
Cardiac Surgery
University of Rostock
Murry CE, Soonpaa MH, Reinecke H, Nakajima H, Nakajima HO, Rubart M, et al. Haematopoietic stem cells do not transdifferentiate
into cardiac myocytes in myocardial infarcts. Nature. 2004 Apr 8;428(6983):664-8.
Cardiac Surgery
University of Rostock
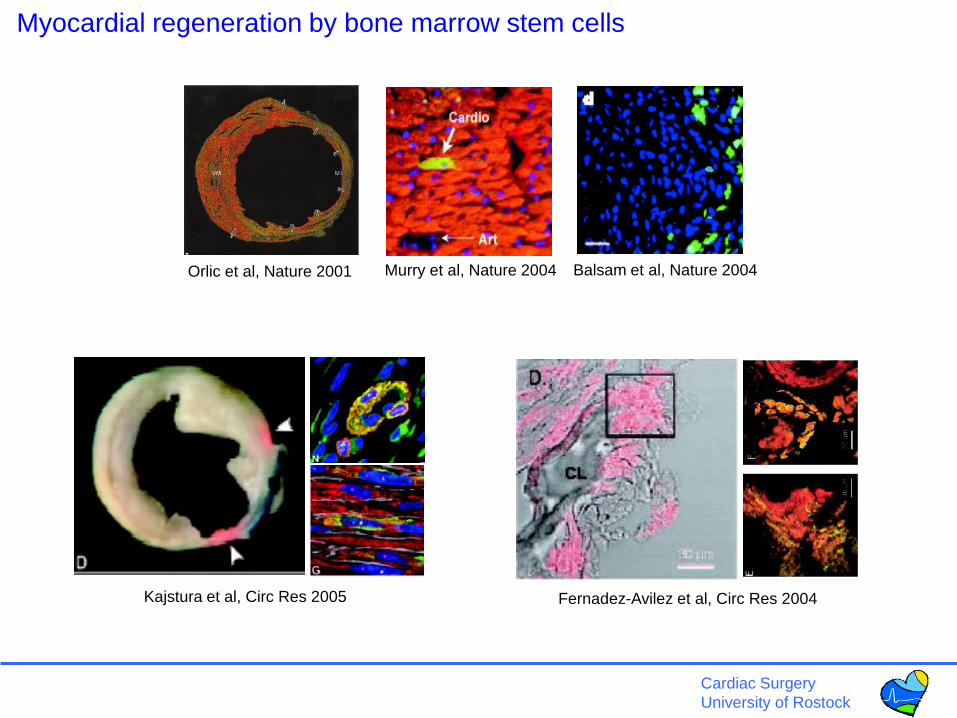
Orlic et al, Nature 2001 Murry et al, Nature 2004 Balsam et al, Nature 2004
Myocardial regeneration by bone marrow stem cells
Fernadez-Avilez et al, Circ Res 2004Kajstura et al, Circ Res 2005
Cardiac Surgery
University of Rostock
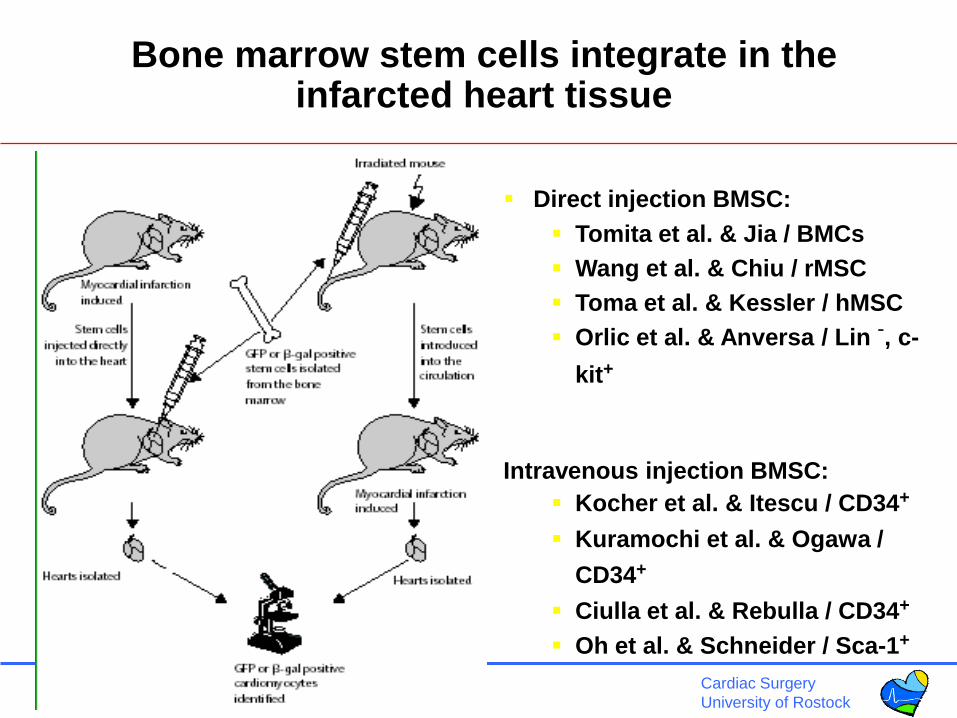
Direct injection BMSC:
Tomita et al. & Jia / BMCs
Wang et al. & Chiu / rMSC
Toma et al. & Kessler / hMSC
Orlic et al. & Anversa / Lin -, c-
kit+
Intravenous injection BMSC:
Kocher et al. & Itescu / CD34+
Kuramochi et al. & Ogawa /
CD34+
Ciulla et al. & Rebulla / CD34+
Oh et al. & Schneider / Sca-1+
Bone marrow stem cells integrate in the infarcted heart tissue
Cardiac Surgery
University of Rostock
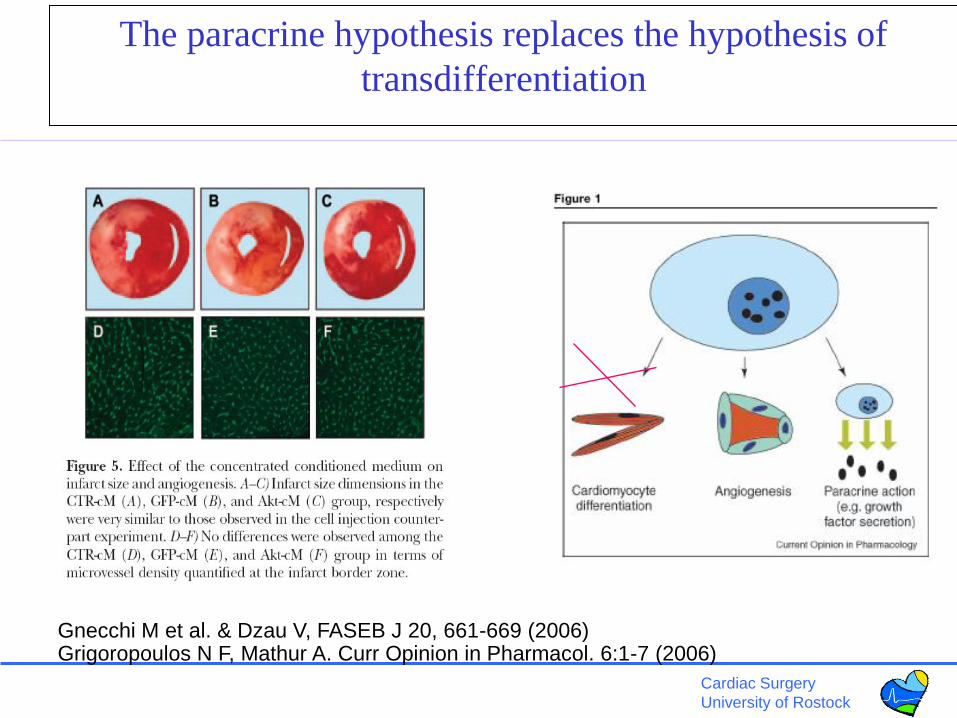
The paracrine hypothesis replaces the hypothesis of
transdifferentiation
Gnecchi M et al. & Dzau V, FASEB J 20, 661-669 (2006)Grigoropoulos N F, Mathur A. Curr Opinion in Pharmacol. 6:1-7 (2006)

Cardiac Surgery
University of Rostock
Embryonic stem cells
Perez-Terzic, Circ Res. 2003, Hodgson et al, AJP 2004
Cardiac Surgery
University of Rostock
Cardiac Surgery
University of Rostock
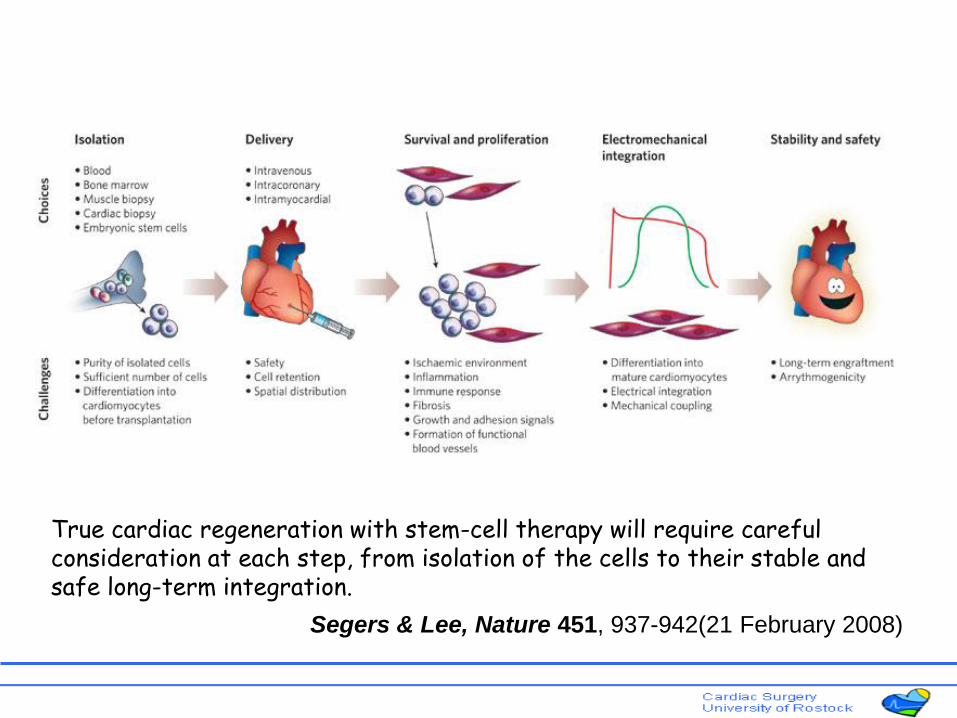
True cardiac regeneration with stem-cell therapy will require careful consideration at each step, from isolation of the cells to their stable and safe long-term integration.
Segers & Lee, Nature 451, 937-942(21 February 2008)
Cardiac Surgery
University of Rostock
Cardiac Surgery
University of Rostock
• Acute myocardial infarction (immediately - days)
• Early after myocardial infarction (< 2 weeks)
• Chronic ischemia: Myocardial transition / remodelling
phase (2 weeks – several months)
• Completed remodelling / scar postischemic
cardiomyopathy (>6 months)
Clinical indication – acute/chronic ischemia, post infarction
Cardiac Surgery
University of Rostock
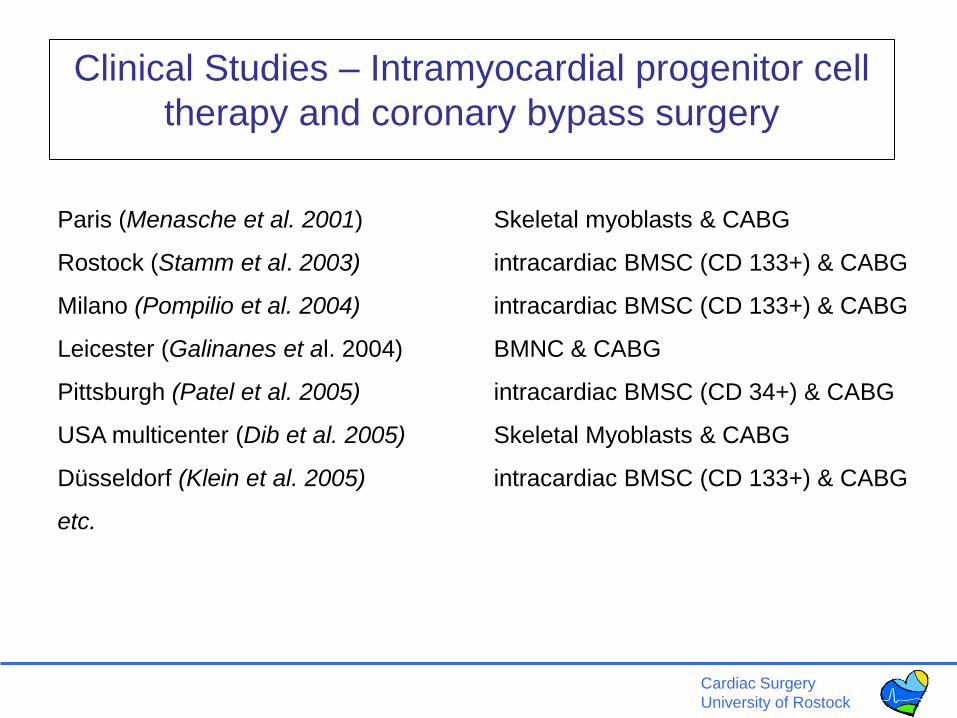
Clinical Studies – Intramyocardial progenitor cell
therapy and coronary bypass surgery
Paris (Menasche et al. 2001) Skeletal myoblasts & CABG
Rostock (Stamm et al. 2003) intracardiac BMSC (CD 133+) & CABG
Milano (Pompilio et al. 2004) intracardiac BMSC (CD 133+) & CABG
Leicester (Galinanes et al. 2004) BMNC & CABG
Pittsburgh (Patel et al. 2005) intracardiac BMSC (CD 34+) & CABG
USA multicenter (Dib et al. 2005) Skeletal Myoblasts & CABG
Düsseldorf (Klein et al. 2005) intracardiac BMSC (CD 133+) & CABG
etc.
Cardiac Surgery
University of Rostock
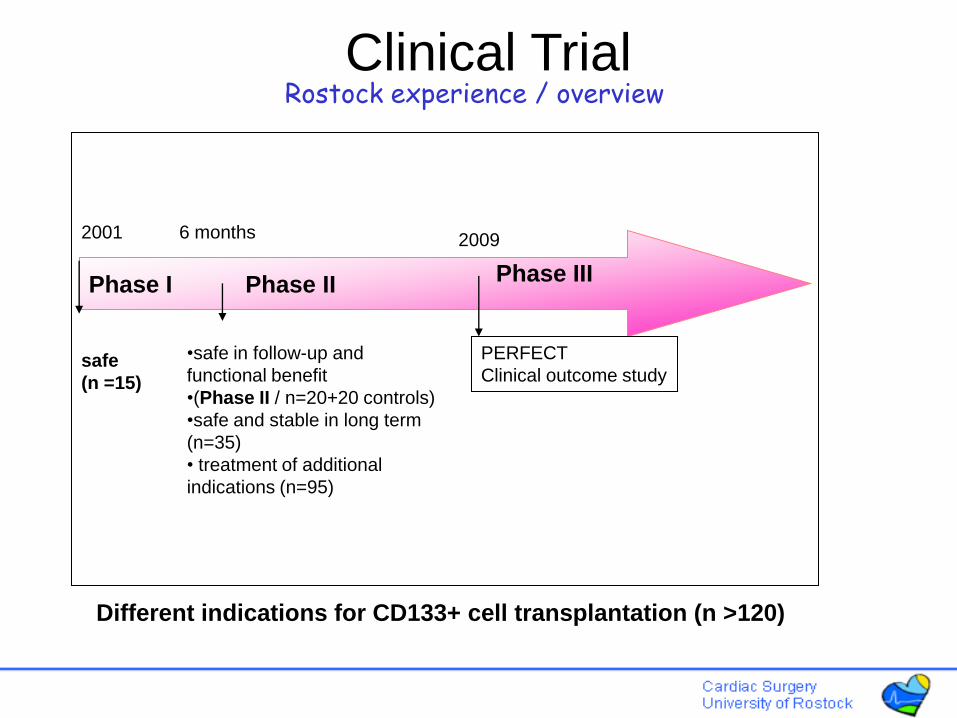
Phase I Phase II
safe
(n =15)
•safe in follow-up and
functional benefit
•(Phase II / n=20+20 controls)
•safe and stable in long term
(n=35)
• treatment of additional
indications (n=95)
2001 2009 6 months
Rostock experience / overview
PERFECT
Clinical outcome study
Clinical Trial
Different indications for CD133+ cell transplantation (n >120)
Phase III

Cardiac Surgery
University of Rostock
Standardization and training of clinical procedures
Characterization of CD133+ as a cellular product
Chest midline
Chest anterolateral
AC133AC133AC133AC133AC133AC133AC133AC133
100 – 200 ml bone marrow aspirate
CliniMACS separation
BMNC preparation
CD133+ labelling
Cardiac Surgery
University of Rostock
10
20
30
40
50
60
70
preop discharge 6 months 18 months
LV
EF
(%
)
399
476*508* 486*
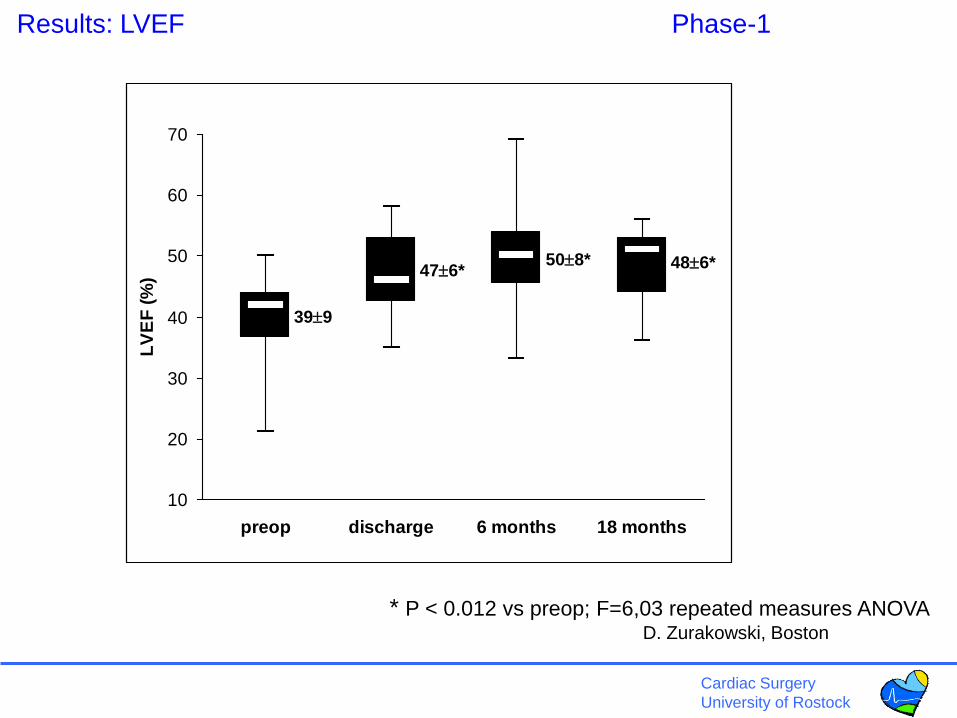
Results: LVEF Phase-1
* P < 0.012 vs preop; F=6,03 repeated measures ANOVAD. Zurakowski, Boston
Cardiac Surgery
University of Rostock
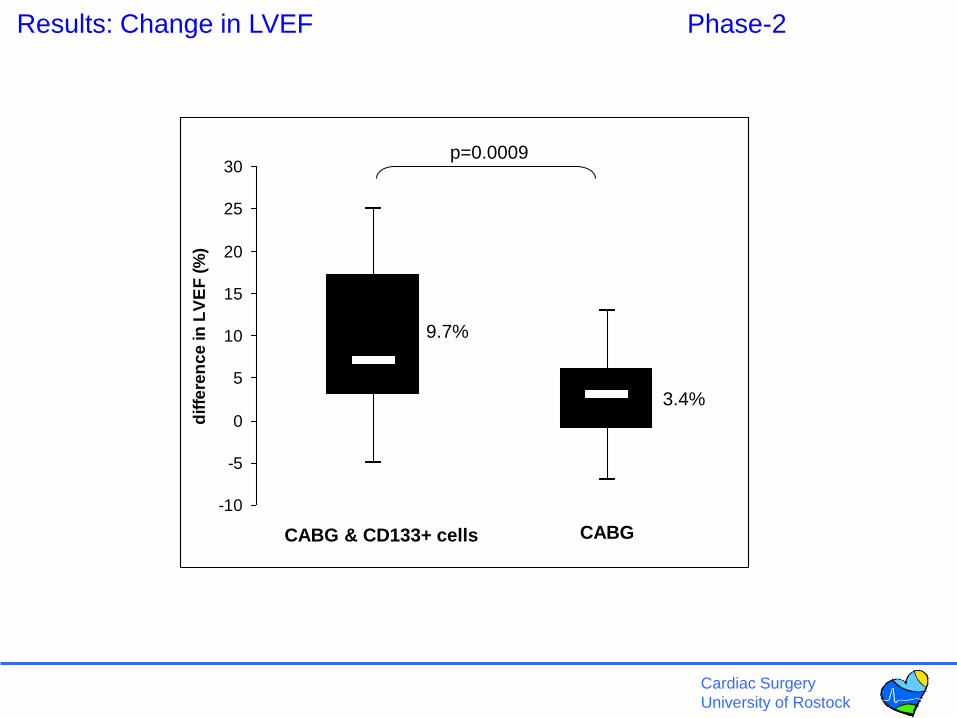
Results: Change in LVEF Phase-2
-10
-5
0
5
10
15
20
25
30
dif
fere
nc
e in
LV
EF
(%
)
CABG & CD133+ cells CABG
9.7%
3.4%
p=0.0009

Cardiac Surgery
University of Rostock
CABG+cells: Effect of preoperative LV function Phase-1 and 2
change in LVEF following CABG & CD133+ cells
-10
-5
0
5
10
15
20
25
30
diffe
ren
ce in
LV
EF
(%
)
< 35% > 35%preop LVEF
15.4%
6.5%
p=0.003
Cardiac Surgery
University of Rostock
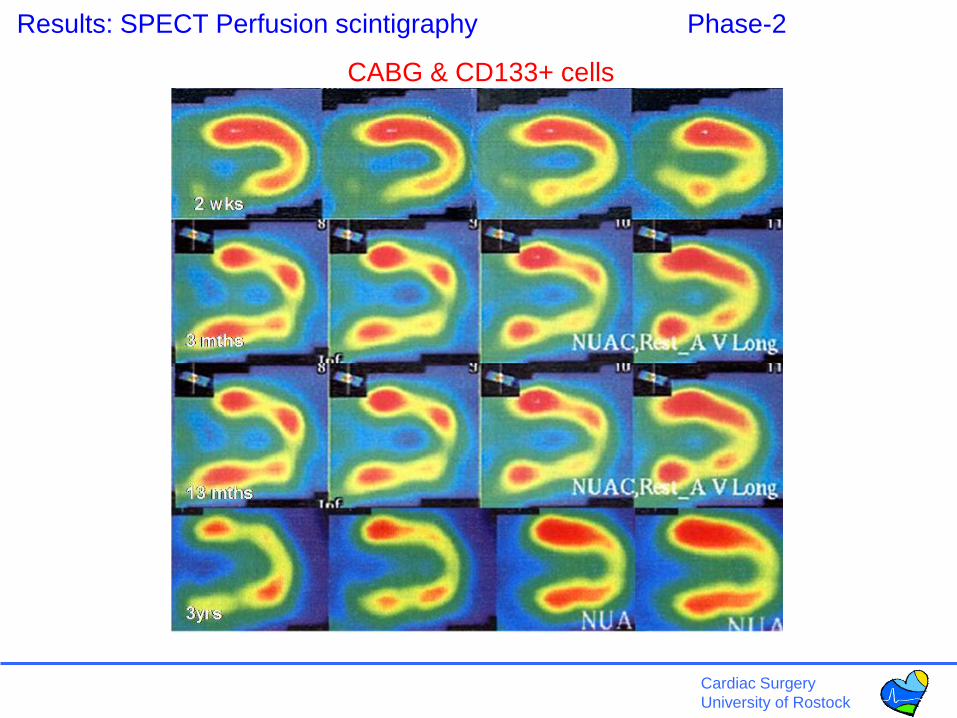
Results: SPECT Perfusion scintigraphy Phase-2
CABG & CD133+ cells
Cardiac Surgery
University of Rostock
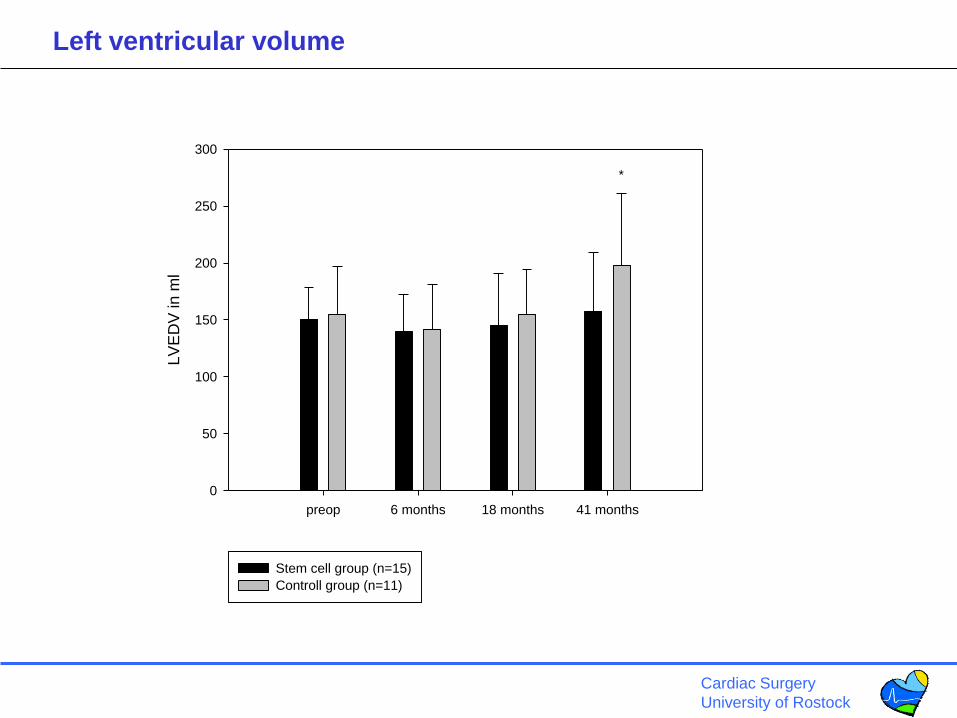
preop 6 months 18 months 41 months
LV
ED
V in
ml
0
50
100
150
200
250
300
Stem cell group (n=15)
Controll group (n=11)
*
Left ventricular volume
Cardiac Surgery
University of Rostock
Current status
• A Phase-I clinical feasibility and safety study in 15 CABG patients showed that intramyocardial injection of autologous CD133+ bone marrow cells was not associated with cell-related complications in longterm analysis 1,2.
• In a subsequent Phase-II randomized, controlled, and prospective clinical trial in 40 patients, CABG & intramyocardial injection of CD133+ bone marrow cells resulted in better LV ejection fraction and perfusion than CABG only 3. Longterm safety of the treatment could be confirmed 4.
• Phase-III clinical study investigation (multicentre double-blinded randomized trial) is planned to start in 2009 for definitive clinical introduction in the treatment of chronic ischemia after myocardial infarction.
1 Stamm et al. Autologous bone marrow stem-cell transplantation for myocardial regeneration. Lancet, 361(9351);45-6; 2003
2 Stamm et al. CABG and bone marrow stem cell transplantation after myocardial infarction. Thorac Cardiov Surg, 52(3):152-8; 2004
3 Stamm et al. Intramyocardial delivery of CD133+ bone marrow cells and coronary artery bypass grafting for chronic ischemic heart
disease: safety and efficacy sturdies. J Thorac Cardiov Surg, 133(3):717-25; 2007
4 Yerebakan et al. Safety of intramyocardial stem cell therapy for the ischemic myocardium: Results of the Rostock trial after five year
follow-up. Cell transplantation 2007; 16(9): 935-40.

Cardiac Surgery
University of Rostock
The impact of stem cells in the future of cardiac therapies
• Stem cells in heart failure treatment
• Stem cells and bridge-to-recovery/ bridge-to-transplant
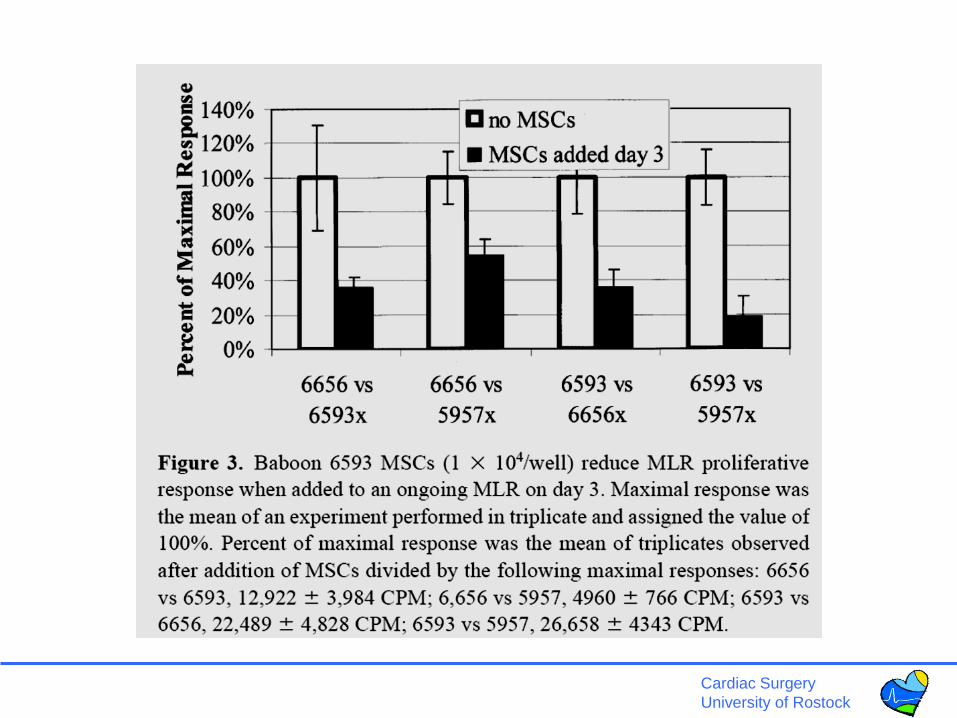
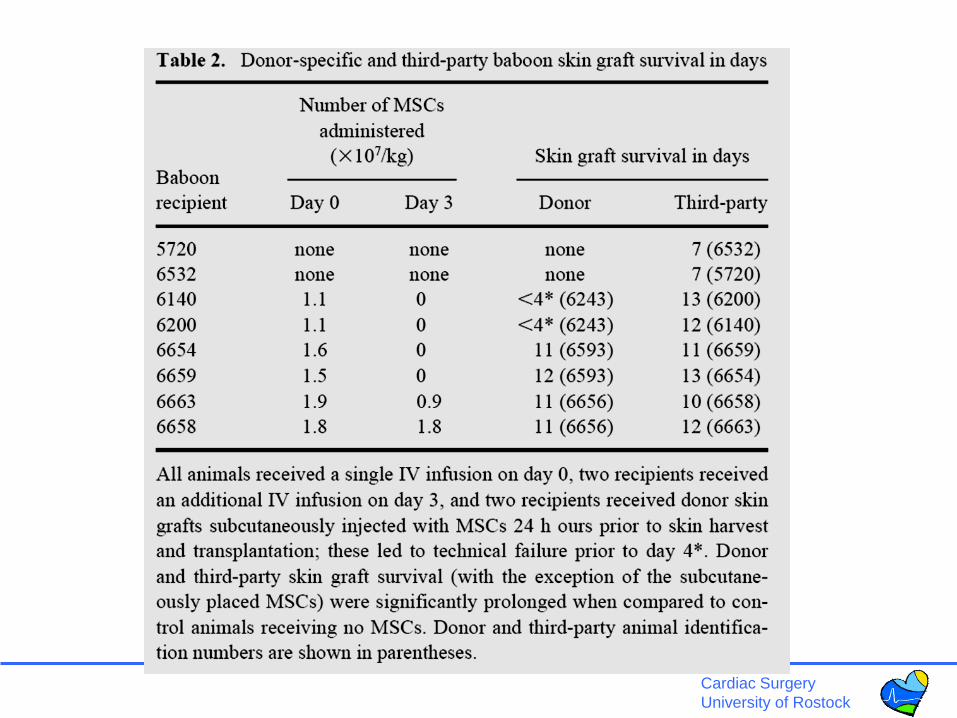
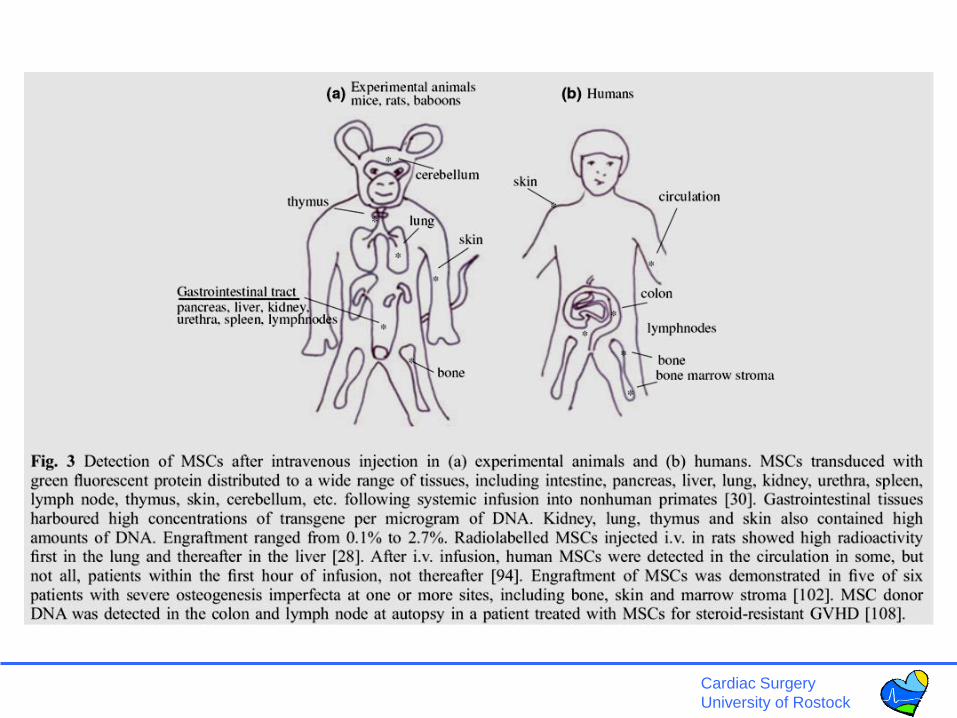
• Stem cells and immunomodulation after heart
transplantation
• Cellular chimerism and cellular renewal in heart
transplants
• Summary and outlook
Cardiac Surgery
University of Rostock
Regenerative options during bridging
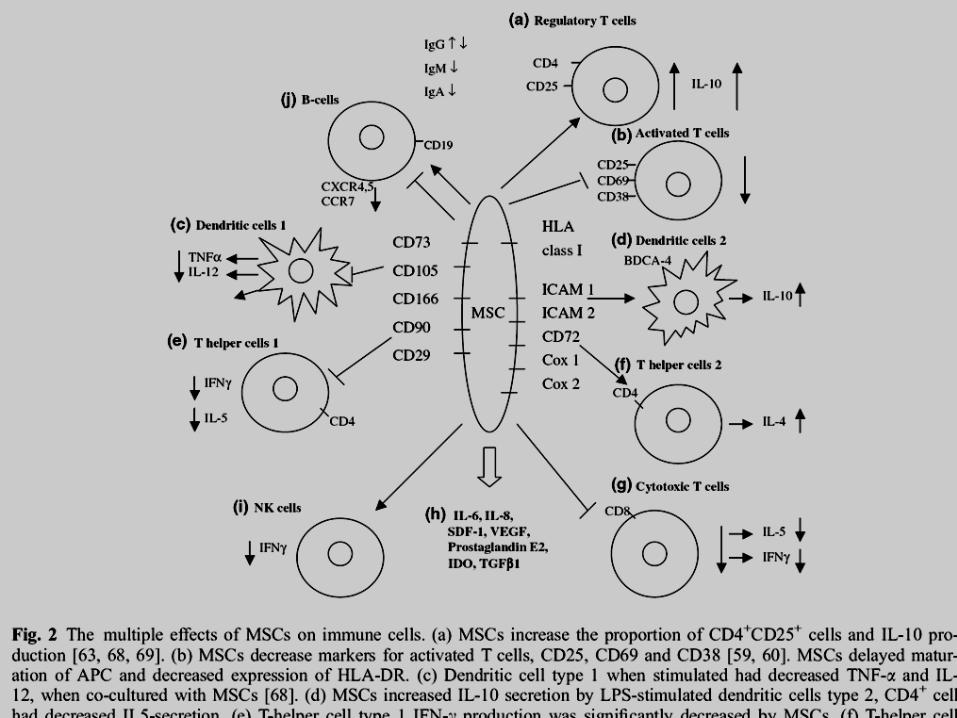
• Immunosuppression (MSC-Treg)
- in viral myocarditis
- in systemic inflammation
• Cardiac regeneration:
- skeletal myoblasts
- HSC, CSC, MSC
- pharmacologic (clenbuterol, EPO)

Cardiac Surgery
University of Rostock
LVAD/stem cell therapy
• Combined autologous cellular cardiomyoplasty using skeletal
myoblasts and bone marrow cells for human ischemic cardiomyopathy
with left ventricular assist system implantation: report of a case.
Miyagawa S, Matsumiya G, Funatsu T, Yoshitatsu M, Sekiya N, Fukui
S, et al. Surgery today. 2009;39(2):133-6.
• Safety and feasibility of autologous myoblast transplantation in patients
with ischemic cardiomyopathy: four year follow-up. Dib N, Michler RE,
Pagani FD, Wright S, Kereiakes DJ, Lengerich R, Binkley P, Buchele
D, Anand I, Swingen C, Di Carli MF, Thomas JD, Jaber WA, Opie SR,
Campbell A, McCarthy P, Yeager M, Dilsizian V, Griffith BP, Korn R,
Kreuger SK, Ghazoul M, MacLellan WR, Fonarow G, Eisen HJ,
Dinsmore J, Diethrich E.
Cardiac Surgery
University of Rostock
The impact of stem cells in the future of cardiac therapies
• Stem cells in heart failure treatment
• Stem cells and bridge-to-recovery/ bridge-to-transplant
• Stem cells and immunomodulation after heart
transplantation
• Cellular chimerism and cellular renewal in heart
transplants
• Summary and outlook
Cardiac Surgery
University of Rostock
Potential of stem cells in heart transplant
patients
• Tolerance induction (BM-Chimerism)
• Immunosuppression (MSC, HLA-G)
• Cellular exchange of donor cells by
recipient SC (EC, IC, Cardiomyoc.)

Cardiac Surgery
University of Rostock
Cardiac Surgery
University of Rostock
Cardiac Surgery
University of Rostock
Cardiac Surgery
University of Rostock
Cardiac Surgery
University of Rostock
Cardiac Surgery
University of Rostock
Cardiac Surgery
University of Rostock
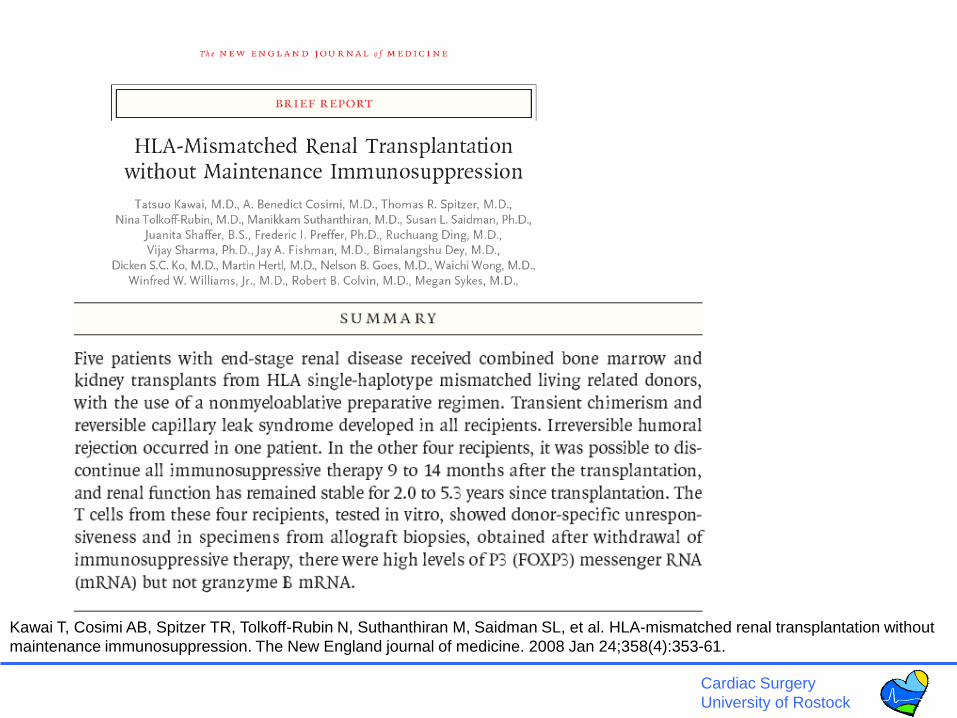
Kawai T, Cosimi AB, Spitzer TR, Tolkoff-Rubin N, Suthanthiran M, Saidman SL, et al. HLA-mismatched renal transplantation without
maintenance immunosuppression. The New England journal of medicine. 2008 Jan 24;358(4):353-61.
Cardiac Surgery
University of Rostock
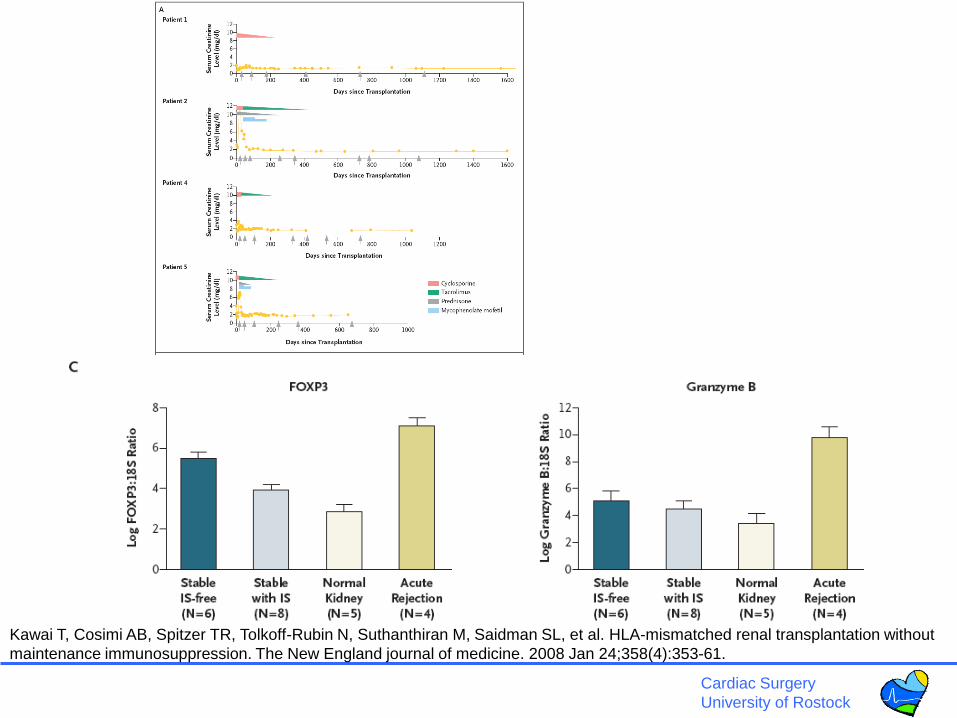
Kawai T, Cosimi AB, Spitzer TR, Tolkoff-Rubin N, Suthanthiran M, Saidman SL, et al. HLA-mismatched renal transplantation without
maintenance immunosuppression. The New England journal of medicine. 2008 Jan 24;358(4):353-61.
Cardiac Surgery
University of Rostock
The impact of stem cells in the future of cardiac therapies
• Stem cells in heart failure treatment
• Stem cells and bridge-to-recovery/ bridge-to-transplant
• Stem cells and immunomodulation after heart
transplantation
• Cellular chimerism and cellular renewal in heart
transplants
• Summary and outlook
Cardiac Surgery
University of Rostock
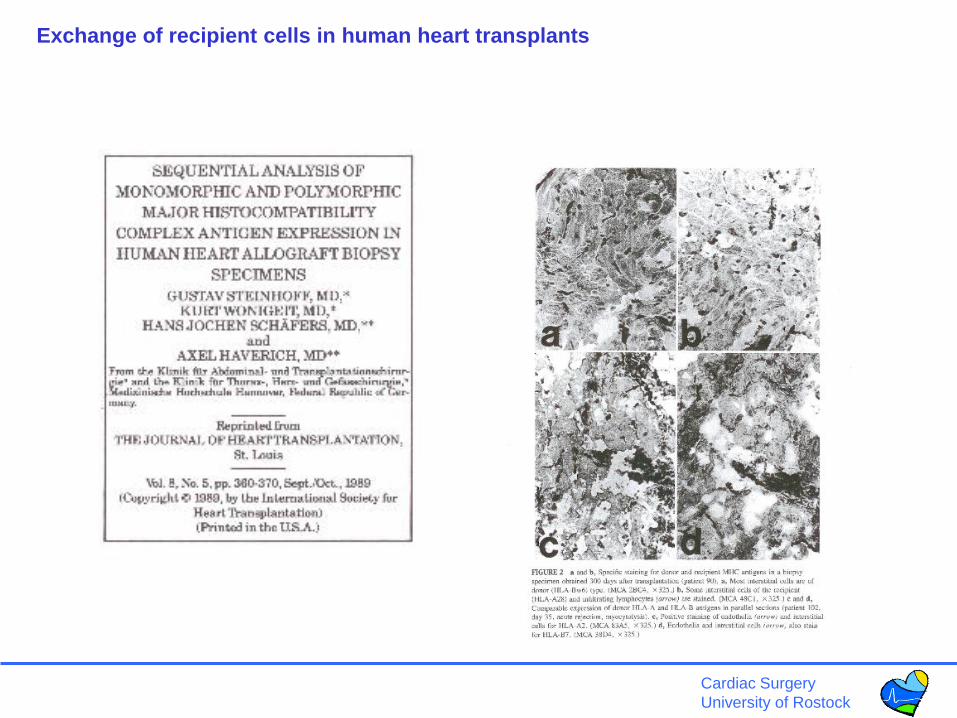
Exchange of recipient cells in human heart transplants

Cardiac Surgery
University of Rostock

Cardiac Surgery
University of Rostock
Thiele J, Varus E, Wickenhauser C, Kvasnicka HM, Lorenzen J, Gramley
F, et al. Mixed chimerism of cardiomyocytes and vessels after allogeneic
bone marrow and stem-cell transplantation in comparison with cardiac
allografts. Transplantation. 2004 Jun 27;77(12):1902-5.
Cardiac Surgery
University of Rostock
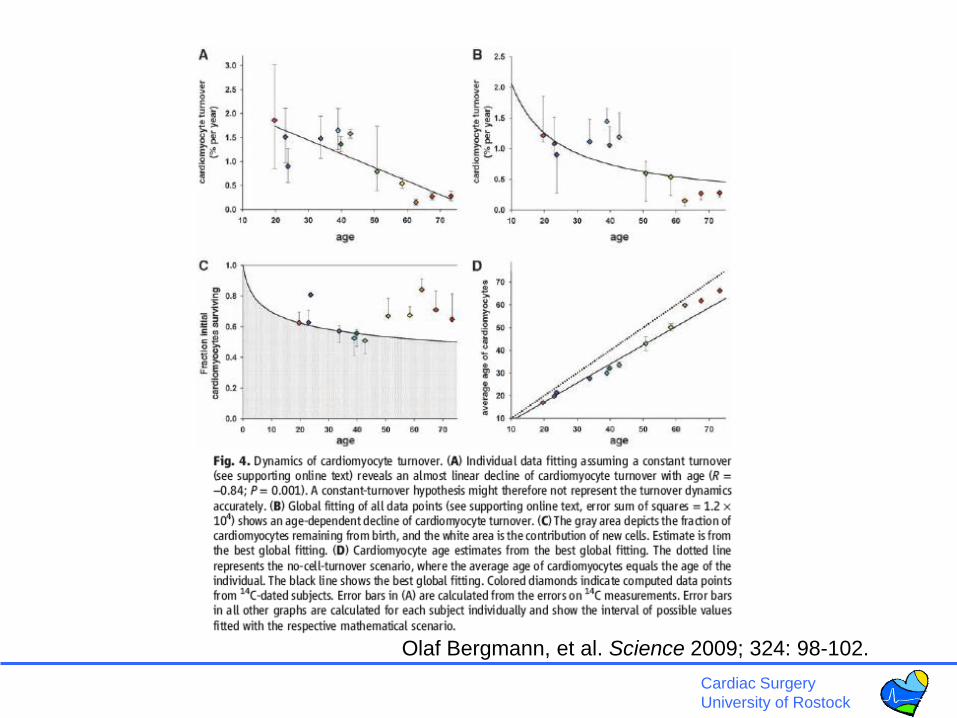
• It has been difficult to establish whether we are limited to the
heart muscle cells we are born with or if cardiomyocytes are
generated also later in life. We have taken advantage of the
integration of carbon-14, generated by nuclear bomb tests during
the Cold War, into DNA to establish the age of cardiomyocytes in
humans. We report that cardiomyocytes renew, with a gradual
decrease from 1% turning over annually at the age of 25 to 0.45%
at the age of 75. Fewer than 50% of cardiomyocytes are
exchanged during a normal life span. The capacity to generate
cardiomyocytes in the adult human heart suggests that it may be
rational to work toward the development of therapeutic strategies
aimed at stimulating this process in cardiac pathologies.
•DOI: 10.1126/science.1164680
•Science 324, 98 (2009);
•Olaf Bergmann, et al.
Turnover after the fallout: Evidence for cardiomyocyte renewal in humans.
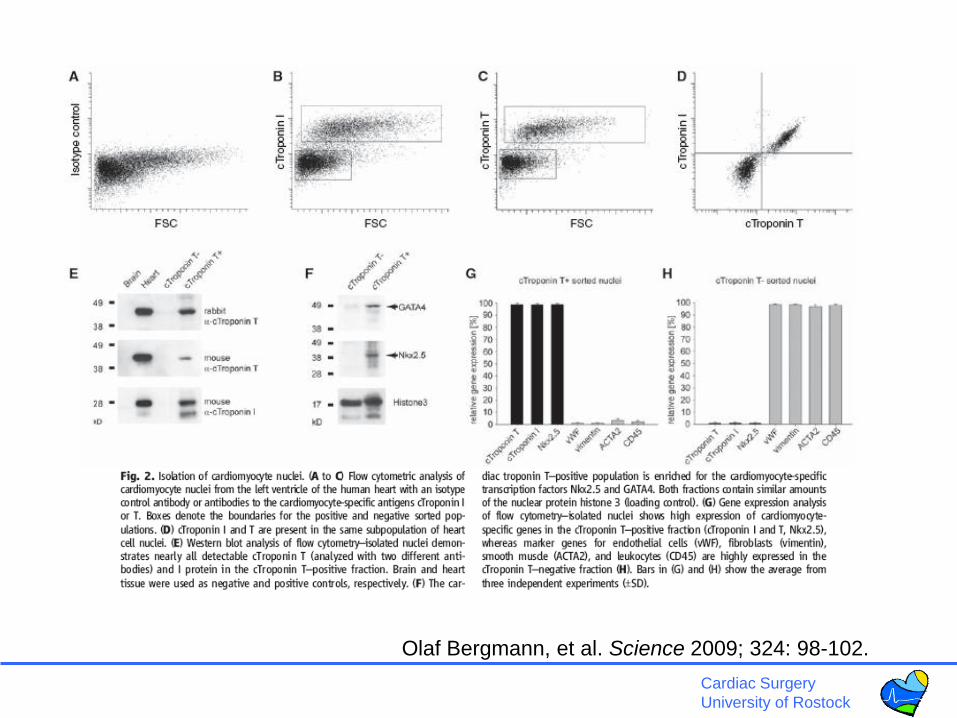
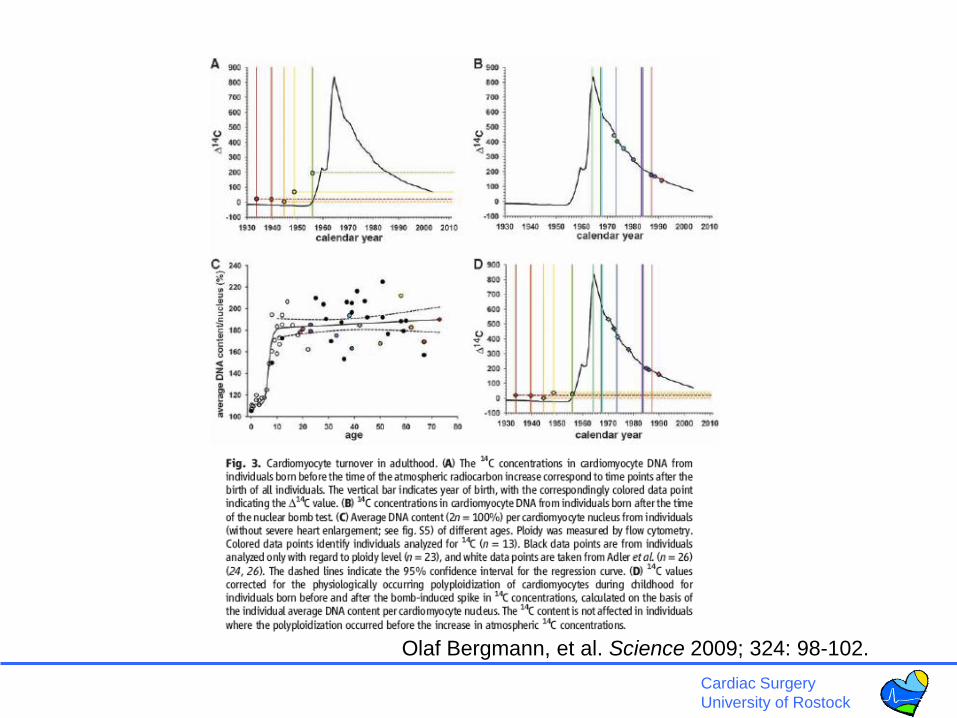
Olaf Bergmann, et al. Science 2009; 324: 98-102.
Cardiac Surgery
University of Rostock
Olaf Bergmann, et al. Science 2009; 324: 98-102.
Cardiac Surgery
University of Rostock
Olaf Bergmann, et al. Science 2009; 324: 98-102.
Cardiac Surgery
University of Rostock
Olaf Bergmann, et al. Science 2009; 324: 98-102.
Cardiac Surgery
University of Rostock

Cardiac Surgery
University of Rostock
Cardiac Surgery
University of Rostock

Cardiac Surgery
University of Rostock
The impact of stem cells in the future of cardiac therapies
• Stem cells in heart failure treatment
• Stem cells and bridge-to-recovery/ bridge-to-transplant
• Stem cells and immunomodulation after heart
transplantation
• Cellular chimerism and cellular renewal in heart
transplants
• Summary and outlook
Cardiac Surgery
University of Rostock
Cardiac Surgery
University of Rostock
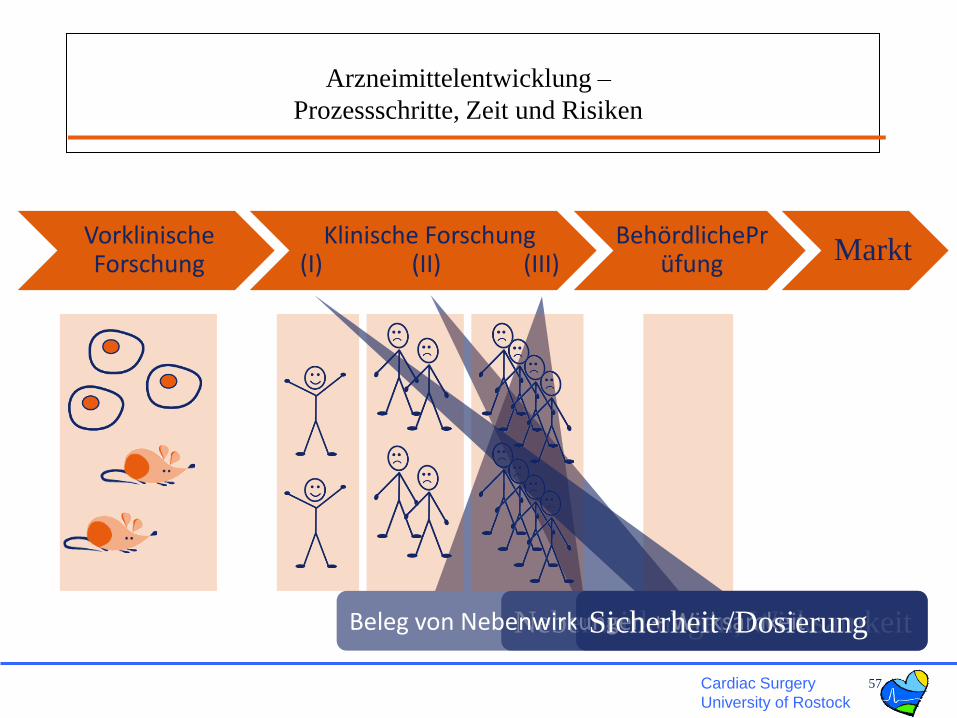
Nebenwirkungen, WirksamkeitBeleg von Nebenwirkungen + Wirksamkeit
Arzneimittelentwicklung –
Prozessschritte, Zeit und Risiken
57
Klinische Forschung(I) (II) (III)
BehördlichePrüfung
Vorklinische Forschung Markt
Sicherheit /Dosierung
Cardiac Surgery
University of Rostock
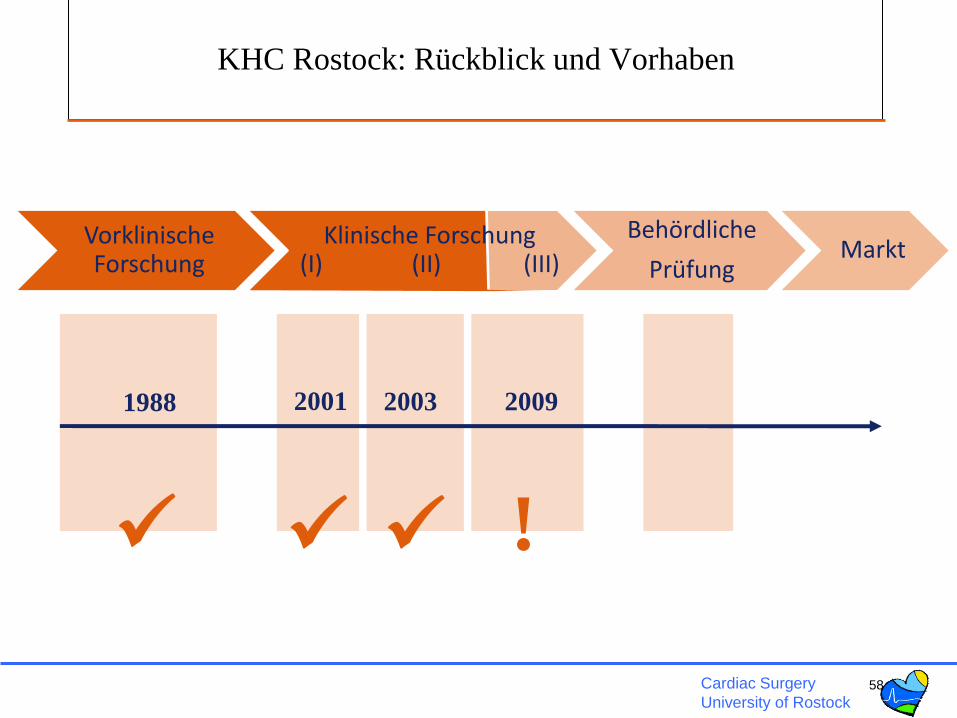
KHC Rostock: Rückblick und Vorhaben
58
Klinische Forschung(I) (II) (III)
Behördliche
Prüfung
Vorklinische Forschung
Markt
2009200320011988
!
Cardiac Surgery
University of Rostock
Im letzten Jahr ….
• Genehmigung der Phase-III-Studie PERFECT
• Aufbau der Kooperation mit den Industriepartnern
(Miltenyi Biotec und Bundesdruckerei/D-Trust)
• Förderzusagen von
– BMBF (Mai 2008): klinische Prüfung, Produktion, F&E und
Entwicklung eines elektronischen Dokumentationssystems
– Ministerium für Wirtschaft, Arbeit und Tourismus M-V
(Okt. 2008): F&E und Innovationsmanagement
• Entscheidung für Aufbau eines Referenz- und Translationszentrums für
kardiale Stammzelltherapie an der Universität Rostock (RTC)
59
Cardiac Surgery
University of Rostock
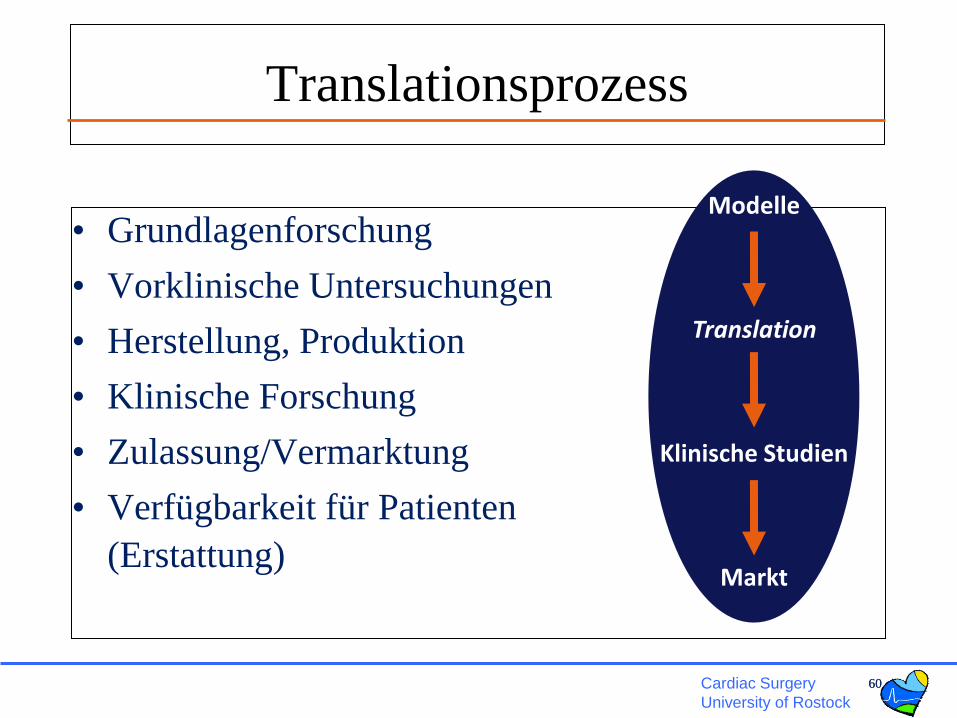
Translationsprozess
• Grundlagenforschung
• Vorklinische Untersuchungen
• Herstellung, Produktion
• Klinische Forschung
• Zulassung/Vermarktung
• Verfügbarkeit für Patienten
(Erstattung)
6060
Modelle
Translation
Klinische Studien
Markt
Cardiac Surgery
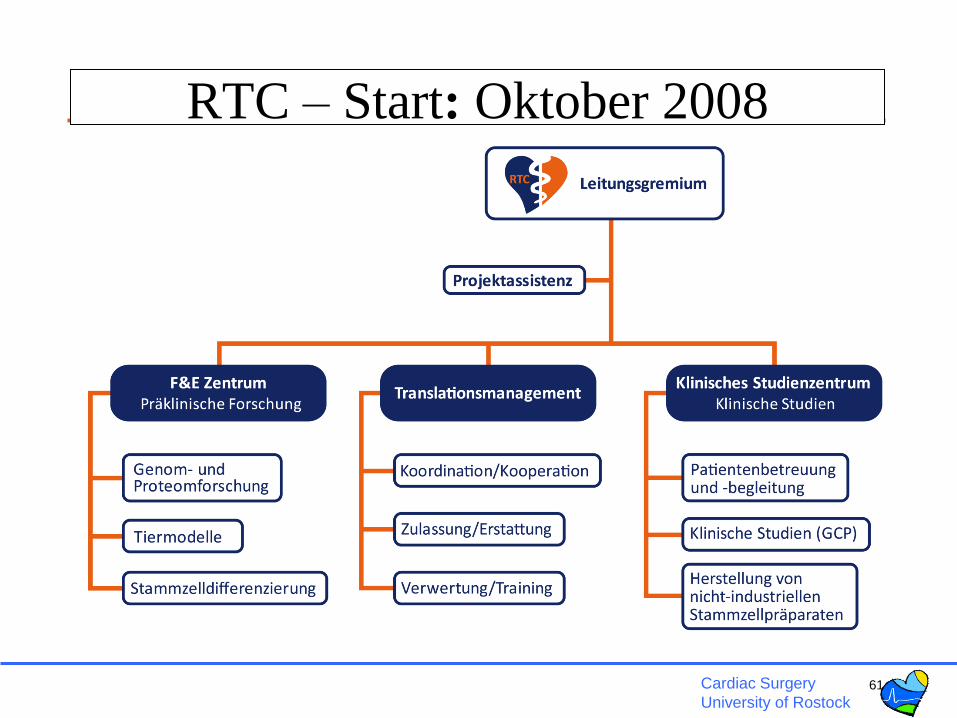
University of Rostock61
RTC – Start: Oktober 2008
Cardiac Surgery
University of Rostock
Leitungsteam
Prof. Dr. Gustav Steinhoff
Dr. Gudrun Tiedemann
Dr. Nan Ma
Priv. Doz. Dr. Klaus Wagner
Prof. Dr. Bodo Eckehard Strauer
62
RTC – Team
Projektassistenz
F & E ZentrumTranslations
managementKlinisches Studienzentrum
Cardiac Surgery
University of Rostock63
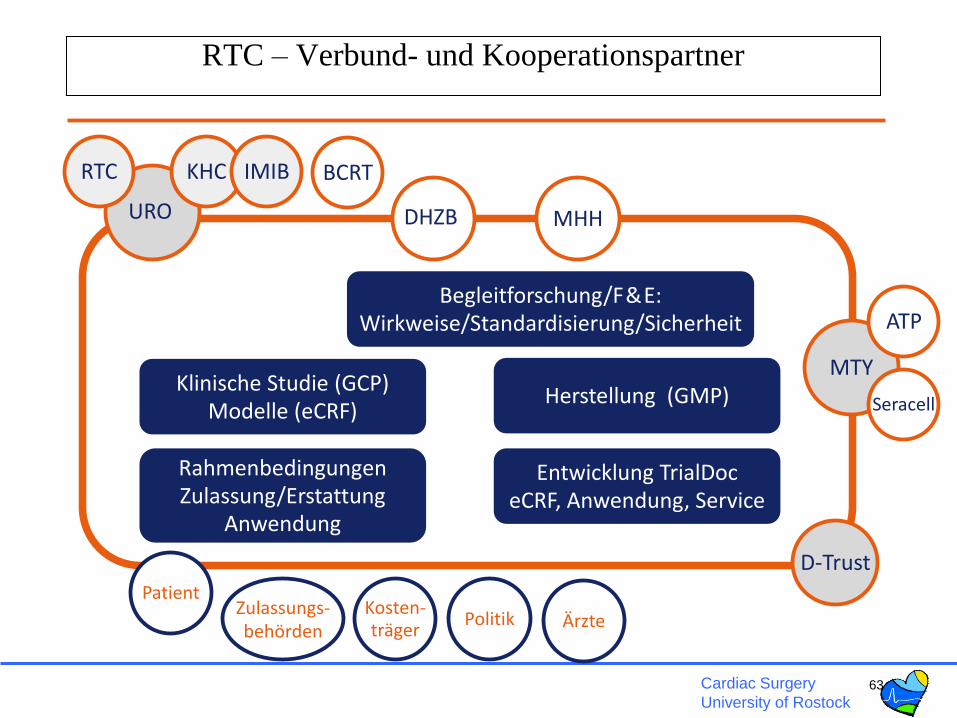
RTC – Verbund- und Kooperationspartner
Klinische Studie (GCP)Modelle (eCRF)
Herstellung (GMP)
RahmenbedingungenZulassung/Erstattung
Anwendung
Begleitforschung/F&E:Wirkweise/Standardisierung/Sicherheit
Zulassungs-behörden
Kosten-träger ÄrztePolitik
Patient
Entwicklung TrialDoceCRF, Anwendung, Service
D-Trust
URO MHHDHZB
BCRTKHCRTC IMIB
MTY
ATP
Seracell

Cardiac Surgery
University of Rostock
Standardization of cardiac stem cell therapy
•Indication
(ischemia/postinfarction/cardiomyopathy/Htx)
•Safety (arrhythmia, tumor, calcification)
•Dosage/Toxicity
•Standardization of cell preparation
•Efficacy (longterm, quality of life)
•Biodistribution of cells (migration, survival)
•Tumorogenicity
•Mechanism of action (paracrine, cellular)
•Comparison of different stem cell types
•CLINICAL OUTCOME (PE,MACE,QoL)

Cardiac Surgery
University of Rostock
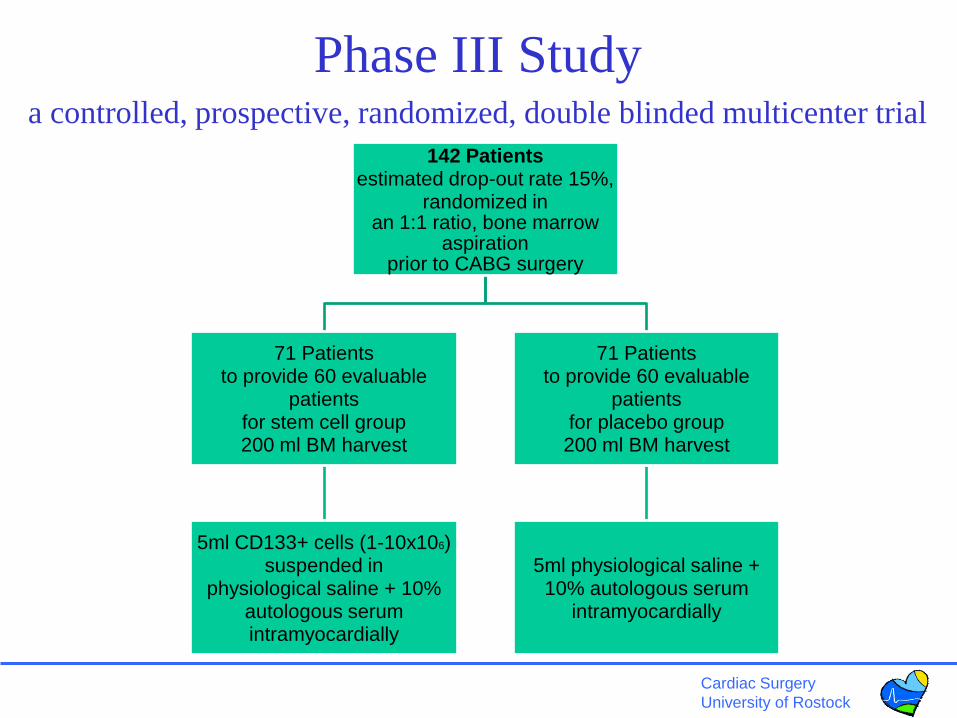
Phase III Studya controlled, prospective, randomized, double blinded multicenter trial
PERFECT
INTRAMYOCARDIAL TRANSPLANTATION OF BONE MARROW STEM CELLS FOR IMPROVEMENT OF POST-INFARCT MYOCARDIAL
REGENERATION IN ADDITION TO CABG SURGERY
Principal investigator: Prof. Dr. G. Steinhoff
Sponsor: Miltenyi-Biotec GmbH
German study centers: Berlin Heart Center
Medical School Hannover
University of Rostock
Approved (Phase III clinical trial) by Paul Ehrlich Institute June 2009
First patient: October 2009
Recruitment: 24 months
Planned final evaluation: 2012
CLINICAL OUTCOME STUDY
Cardiac Surgery
University of Rostock
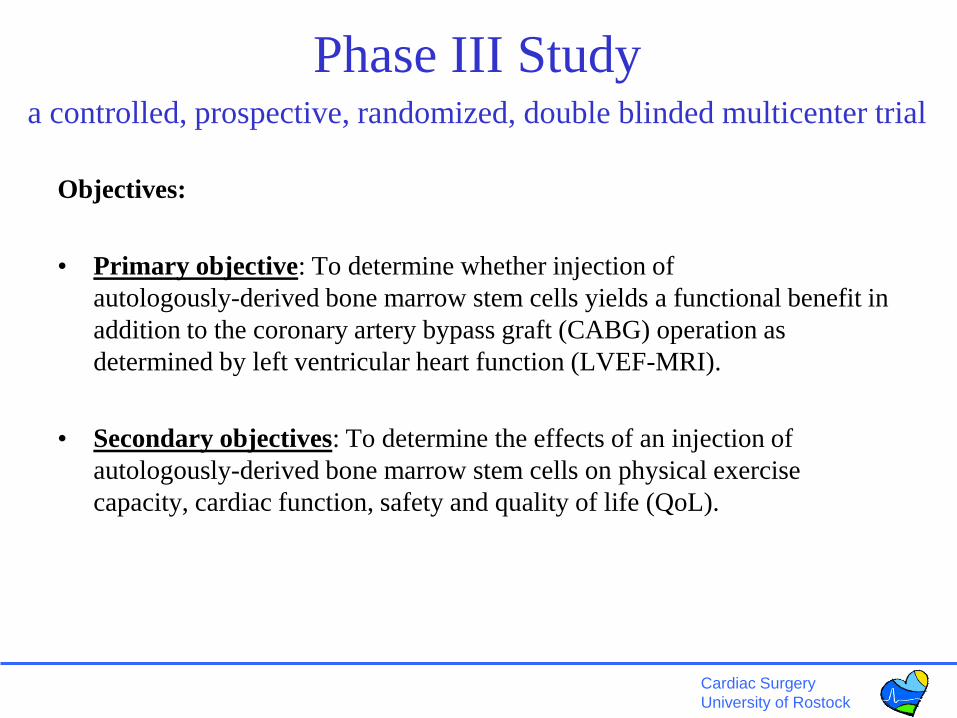
Objectives:
• Primary objective: To determine whether injection of
autologously-derived bone marrow stem cells yields a functional benefit in
addition to the coronary artery bypass graft (CABG) operation as
determined by left ventricular heart function (LVEF-MRI).
• Secondary objectives: To determine the effects of an injection of
autologously-derived bone marrow stem cells on physical exercise
capacity, cardiac function, safety and quality of life (QoL).
Phase III Studya controlled, prospective, randomized, double blinded multicenter trial
Cardiac Surgery
University of Rostock
Phase III Studya controlled, prospective, randomized, double blinded multicenter trial
142 Patientsestimated drop-out rate 15%,
randomized in an 1:1 ratio, bone marrow
aspiration prior to CABG surgery
71 Patientsto provide 60 evaluable
patientsfor stem cell group200 ml BM harvest
5ml CD133+ cells (1-10x106) suspended in
physiological saline + 10% autologous serumintramyocardially
71 Patientsto provide 60 evaluable
patientsfor placebo group200 ml BM harvest
5ml physiological saline + 10% autologous serum
intramyocardially
Cardiac Surgery
University of Rostock
R&D Partners:
Miltenyi Biotec GmbH
Balshüsemann/Hennemann/Pinkernell
Bergisch-Gladbach/Teterow
D-Trust, Berlin
ATP, Rostock
Helmholtz (GKSS/Teltow)
Clinical Development Partners
Haverich, MH Hannover
Hetzer/Stamm, DHZ Berlin
Management team
Dr..Tiedermann
Ms. Jana Gabriel
Prof. B.E. Strauer
Cardiac Surgery
Andreas Liebold
Alexander Kaminski
Can Yerebakan
Bernd Westphal
Peter Donndorf
Catharina Nesselmann
Ch. Klopsch
Lab/Institute of Regenerative Medicine (RTC/IRMED)
Ma Nan, P. Mark
Wenzhong Li, Ou, Y. Wang
D. Furlani, R. Gäbel, W. Wang
Intenational Partners
NU Singapur,
Beijing/Hefei/Nankai, China
Asahara, CDB/RIKEN, Kobe, Japan
RenkeLiToronto, Kanada;
Capogrossi, IDI, Rome, Italy
Pompilio, Milano, Italy
Department of Cardiac Surgery
University of Rostock
www.cardiac-surgery-rostock.com
www.cardiac-stemcell-therapy.com
This work was supported by the Helmholtz Gemeinschaft, Mecklenburg-Vorpommern (Nachwuchsgruppe
Regenerative Medizin Regulation der Stammzellmigration 0402710), BMBF BioChance PLUS (0313191),
Miltenyi Biotec, Sonderforschungsbereich/Transregio 37, B5, B2 and A4; and BMBF Reference and
Translation Center of Cardiac Stem Cell Therapy (2008-2011).
Cardiac Surgery
University of Rostock
Untertitel
Klinik für Herzchirurige, Universität Rostock, www.herzchirurgie-rostock.de
www.cardiac-stemcell-therapy.com
www.cardiac-surgery-rostock.com
Department of Cardiac Surgery
Medical Faculty
University of Rostock




![Apparative Diagnostik der Dysphagie mittels FEES · [Dziewas et al. 2004, Mann et al. 1999, Smithard et al. 1996] ... [Wu et al. Laryngoscope 1997, Crary et al. Dysphagia 1997, Leder](https://cdn.vdokument.com/doc/165x107/5b6080ae7f8b9a40488b563b/apparative-diagnostik-der-dysphagie-mittels-fees-dziewas-et-al-2004-mann.jpg)


