komplikationen vor und nach sedierung in der gi...
TRANSCRIPT

Komplikationen der Sedierung
bei der GI-Endoskopie
Till Wehrmann
FB Gastroenterologie
Deutsche Klinik für Diagnostik
24. Tagung der NDGG – 14.02.2014

Relevanz Sedierungs-assoziierter
Komplikationen in der GI-Endoskopie
1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010
0
50Abgeschlossene Anträge
Sedierungs- Endoskopie-
assoziiert assoziiert
Diagnostisch 60 % 40 %
Interventionell 30 % 70 %

Sicherheit der Sedierung
in der Endoskopie Komplikations- und Mortalitätsdaten aus Registerstudien
Setting N „Komplikation“ Mortalität
Rex et al., 2009 amb./stationär 422.424 0.0006 % 1:100.000
Frieling et al., 2013 stationär 191.142 0.005 % 3:100.000
Behrens et al., 2013 stationär 388.404 0.01 % 5:100.000
Komplikations- und Mortalitätsdaten aus prospektiven Fallserien
Setting N „Komplikation“ Mortalität
Wehrmann, 2008 nur Intervention 9.547 1.2 % 30:100.000
Behrens, 2013* stationär 73.941 2.2 % ?
*: Interimanalyse, Abstrakt DGVS 2013
Risikosituationen: 1. Notfall 2. Intervention 3. ASA ≥ III

0
5000
10000
15000
20000
25000
Endoscopies, n Sedation, % x 10-6
Patient
sex, age
ASA-
Classification
Sedation Indication for Endoscopy Complication Additional
person for
NAAP
Male
76 years
III 2.5 mg Midazolam
80 mg Propofol
Emergency
GI-Bleeding
Respiratory
Insufficiency
Hypotension
present
Male
75 years
III 1.0 mg Midazolam
40 mg Propofol
Emergency
GI-Bleeding
Respiratory
Insufficiency
Hypotension
present
Female
73 years
III 120 mg Propofol Emergency
GI-Bleeding
Cardiac arrest present
Male
79 years
III 70 mg Propofol Tube feeding Respiratory
Insufficiency
Hypotension
present
Female
84 years
III 1.0 mg Midazolam
120 mg Propofol
Percutaneous endoscopic
gastrostomy
Respiratory
Insufficiency
Hypotension
present
Male
71 years
III 2.5 mg Midazolam
400 mg Propofol
0.5 mg Flumazenil
Transgastral drainage of
infectious pancreatic
pseudocyst
Respiratory
Insufficiency
Hypotension
present
HELIOS-Studie:
Sedierungs-assoziierte Komplikationen
T Frieling et al., Z Gastroenterol 2013; 51: 568-72

Komplikationen der Propofol-Sedierung
bei intervent. EndoskopieParameter Fälle mit
Komplikation / alle
Fälle
P Fälle mit
intensivpflichtiger
Komplikation / alle
Fälle
P
Alter < 70 Jahre 88 / 6684 18 / 6684
Alter 70 Jahre 47 / 2863 0.26 10 / 2863 0.65
BMI < 30 123 / 8784 25 / 8784
BMI 30 12 / 763 0.83 3 / 763 0.86
Patienten ohne
Alkoholabusus
108 / 8402 16 / 8402
Patienten mit
Alkoholabusus
27 / 1145 0.007 12 / 1145 0.003 *
Patienten ohne
Narkotika-
Gebrauch
122 / 8885 26 / 8885
Patienten mit
Narkotika-
Gebrauch
13 / 662 0.29 2 / 662 0.97
ASA: I-II 42 / 6587 13 / 6587
ASA: III-IV 93 / 2960 0.0001 * 15 / 2960 0.02
Elektive
Indikation
47 / 8947 8 / 8974
Notfall-
Indikation
88 / 573 0.0001 * 20 / 573 0.0001 *
Propofol-Dosis
100 mg
31 / 3724 1 / 3724
Propofol-Dosis
> 100 mg
104 / 5823 0.0002 * 27 / 5823 0.0003 *
Mono-
Sedierung
38 / 3151 9 / 3151
Ko-Medikation
mit Midazolam
97 / 6396 0.27 19 / 6396 0.92
T Wehrmann, A Riphaus. Scand J Gastroenterol 2008; 43: 368-74
Parameter Total Fälle mit Komplikationen
Anzahl endoskopischer
Interventionen
9.547 135
Anzahl Patienten 8.735 134
Alter (Jahre, MW±SD [range]) 60.5 ± 29.5 [17-98] 63.4 ± 16.7 [30-93]
Geschlecht (weibl. / männl.) 5201 w / 3534 m 54 w / 80 m a
ÖGD: Blutstillungs- Prozeduren (n) 4.252 72 b
ÖGD: Bougierung/Dilatation 666 3
ÖGD: Stent-Implantation (n) 95 1
ÖGD: EMR-Prozeduren (n) 361 1
EUS-FNA (n) 186 0
EUS-Zysten-Drainage (n) 50 1
ERCP-Interventionen (n) 3.937 56
Komplikationen N
vorzeitiger Abbruch 117 [1.2%]
Maskenbeatmung 40 [0.4%]
Intubation 9 [0.09%]
Intensivmedizin 28 [0.3 %]
Tod 3 [0.03 %]
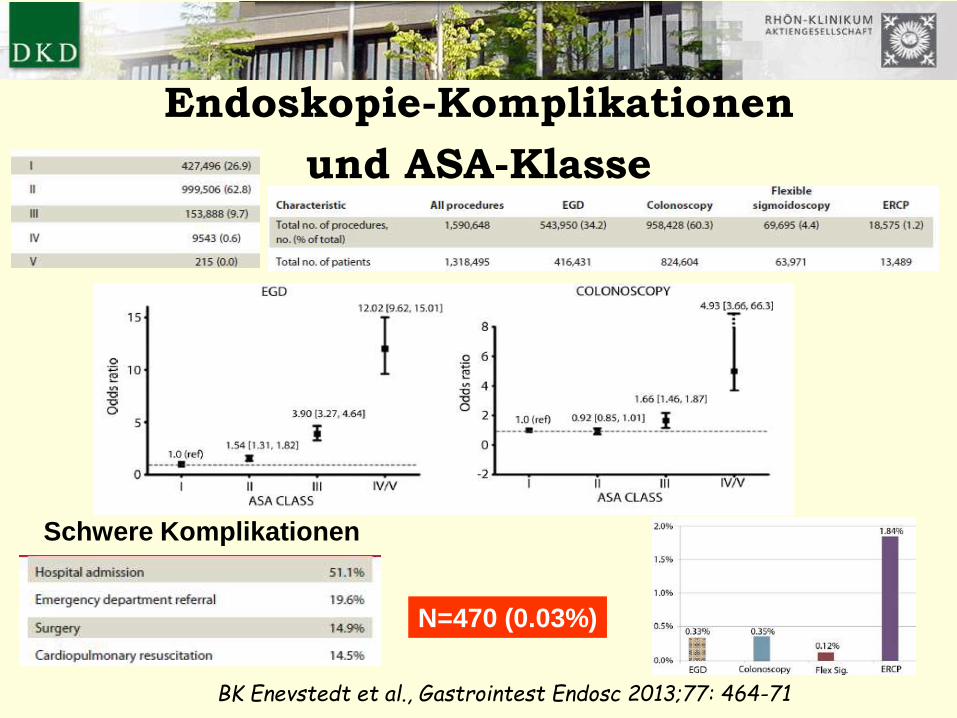
Endoskopie-Komplikationen
und ASA-Klasse
BK Enevstedt et al., Gastrointest Endosc 2013;77: 464-71
N=470 (0.03%)
Schwere Komplikationen
Sedierungskomplikationen vermeiden ?
RISIKO-STRATIFIZIERUNG
GEEIGNETE PERSONELLE RESSOURCEN
GEEIGNETE TECHNISCHE RESSOURCEN
KOMPLIKATIONS-MANAGEMENT
PERSONELLE QUALIFIKATIONEN
TECHNISCHE RESSOURCEN

Alternative: Unsedierte Untersuchung
Reduktion der Friktion
Dünnere Instrumente
[transnasale ÖGD/Gastrokop/Päd. Endoskop]
Variable Versteifung
Kappen-Koloskopie
Psychische Ablenkung
Musikbeschallung
Hypnoseverfahren
Reduktion der Wanddistension
CO2-Insufflation
Wasserinstillation
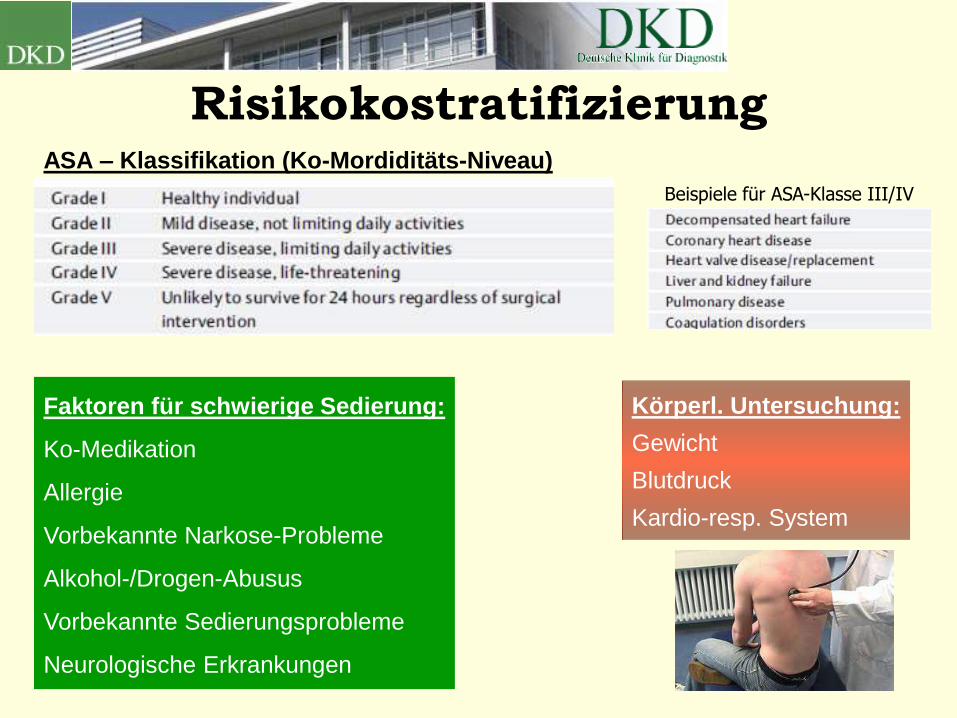
RisikokostratifizierungASA – Klassifikation (Ko-Mordiditäts-Niveau)
Faktoren für schwierige Sedierung:
Ko-Medikation
Allergie
Vorbekannte Narkose-Probleme
Alkohol-/Drogen-Abusus
Vorbekannte Sedierungsprobleme
Neurologische Erkrankungen
Beispiele für ASA-Klasse III/IV
Körperl. Untersuchung:
Gewicht
Blutdruck
Kardio-resp. System

Lokale Risikofaktoren für
schwieriges Atemwegs-Management
Risikofaktoren für kardio-respirat. Probleme während der Endoskopie
Anamnese: Bekannte Narkoseprobleme, Schnarchen,
Schlaf-Apnoe-Syndrom, HWS-Trauma
Körperl. Befund: Stridor, Adipositas, kurzer Hals, Mikrognathie, Trismus
nach: Am Soc Anaesth, Anaesthesiology 1996; 84: 459-71
Hyoid-Kinnspitzen Distanz < 4 cm
Mallampati-Klasse 3-4
Nach: S Mallampati et al., Can Anaesth Soc J 1985

Personelle Ressourcen:gem. Sedierungs-Leitlinie 2008
ASA I-III und
Keine Atemwegsrisiken
und
Einfache Prozeduren
ASA IV/V oder
Atemwegsrisiken oder
Komplexe Prozeduren
Arzt-Endoskopie
Pflege-Endoskopie
Arzt-Sedierung
Arzt-Endoskopie
Pflege-Endoskopie
Anästh.-Sedierung
Arzt-Endoskopie
Pflege-Endoskopie
Anästh.-Sedierung
Pflege-Sedierung
Arzt-Endoskopie
Pflege-Endoskopie
2. Pflege-Endoskopie
Arzt-Sedierung
Arzt-Endoskopie
2. Arzt-Endoskopie
Pflege-Endoskopie
Anästh.-Sedierung
Pflege-Sedierung
Arzt-Endoskopie
Pflege-Endoskopie
2. Pflege-Endoskopie
Anästh.-Sedierung
Pflege-Sedierung
Arzt-Endoskopie
Pflege-Sedierung
Arzt-Endoskopie
Pflege-Endoskopie
Pflege-Sedierung
Arzt-Endoskopie
Pflege-Endoskopie
Arzt-Sedierung
Evidenzlage: Personelle Struktur 2000-2012
-Prospektive Studien und/oder RCT-
Struktur Anzahl Studien Anzahl Patienten
E-DPS (n=2) 1 (Külling, GIE 2007) 27.000 (ÖGD/Kolo)
E-DPS (n=3) 3.173 500.000
NAAP (n=3) 1.876 350.000
MAC (n=?) 88 23.800

Personelle Ressourcen und
Sed.komplikationen
CG Dietrich et al., Scand J Gastroenterol 2013; 48: 1082-7
5/2008-4/2010: 2-/3-Mann; n=6.910
5/2010-4/2012: 3-Mann; n=6.837
*: p=0.03
*: p=0.07
*: p=0.06
FAZ 19.12.13

MAC und Sedierungskomplikationen
M Agostini et al., Gastrointest Endosc 2011; 74: 266-75
N=17.542
8-Jahres-Periode
Komplikationen N (9.547)
Hypotension 190 [2.0%]
O2-Abfall 143 [1.4 %]
Intubation 9 [0.09%]
Mortalität 3 [0.03 %]T Wehrmann, Scand J Gastroenterol 2008
Notfall: 2 %Gesamt 792 [4.5 %]
Hypotension 312 [1.8 %]
Sätt.abfall 217 [1.2 %]
Bradykardie 204 [1.2 %]
Intubation 7 [0.04 %]
Mortalität 3 [0.02 %]
Wann anaesthesiologische Hilfe ?
Bei Patienten mit höherem Risikoprofil soll die Hinzuziehung eines
Anästhesisten erwogen werden, dazu gehören: hohe ASA-
Klassifikation (III-IV) und schwierige endoskopische Eingriffe oder
wenn durch pathologisch-anatomische Besonderheiten des Patienten
ein erhöhtes Risiko für eine Atemwegsbehinderung während des
Eingriffs gegeben ist (z.B. bei kranio-facialen Missbildungen, Tumoren
des Zungengrundes, Larynx oder Hypopharynx, massiv
eingeschränkter Beweglichkeit der HWS, massiv eingeschränkter
Mundöffnung < 3cm, Mallampatti-Stadien 3 oder 4 bzw.
eingeschränkter Kehlkopf-Kinnspitzen Abstand von weniger als 6 cm).
Empfehlungsgrad: A, Evidenzstärke 5, Konsens

Technische Ausstattung
Komplikationsmanagement I
Medikamente
Intubationsbesteck
Beatmungsbeutel
Defibrillator
Absaugpumpe
Larynxmaske

Komplikationsmanagement IIQualifiziertes und trainiertes Personal
Esmarch-HandgriffMaskenbeatmung
CPR, Intubation, BeatmungSimulatortraining
Endoscopy 2013; 45: 496–504

VIELEN DANK
FÜR IHRE AUFMERKSAMKEIT!