patient blood management (pbm)
TRANSCRIPT
Abteilung für Anästhesiologie und Intensivmedizin, AKH Linz
Patient Blood Management
H. Gombotz
Patient Blood Management
„Patient Blood Management (PBM)“ ist ein multidiziplinäres, evidenzbasiertes
Behandlungsmodell, welches zum Ziel hat, durch optimale Behandlung des
patientInneneigenen Blutvolumens die Verabreichung von Fremdblut- und
Fremdblutprodukten bei akzeptablem Anämierisiko auf ein Minimum zu
reduzieren oder gar zu vermeiden.
Mit dem PBM Konzept können Transfusionen nicht ganz vermieden, aber –
geht man vom derzeitigen Verbrauch aus – deutlich reduziert werden.
Damit werden nicht nur die Nebenwirkungen der Bluttransfusion verhindert,
sondern auch die Risiken einer vorbestehenden oder neu auftretenden
Anämie auf ein Minimum reduziert.
3
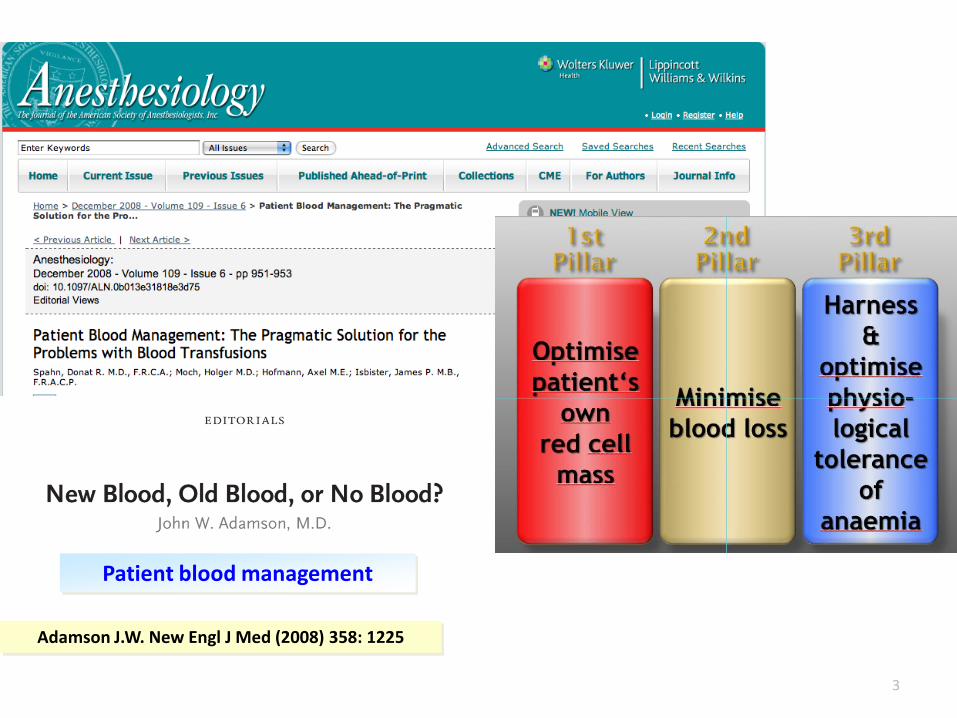
Patient blood management
Adamson J.W. New Engl J Med (2008) 358: 1225
© Axel Hofmann AIC Graz 09-2010
© Axel Hofmann AIC Graz 09-2010
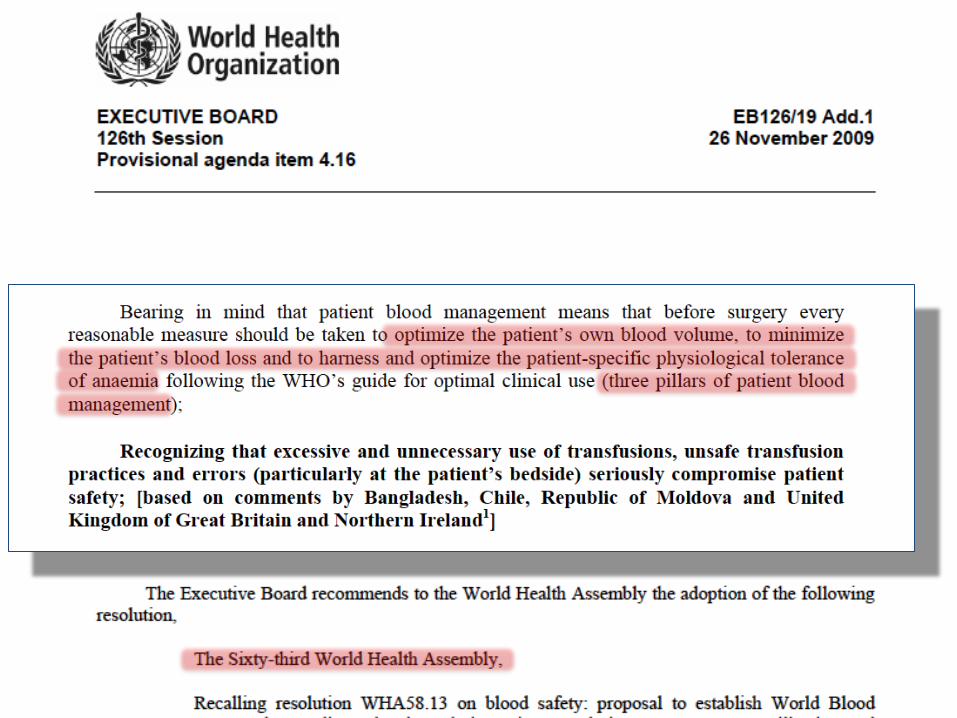
To implement this resolution, the WHO Blood Transfusion Safety Programme
(WHO/BTS), in collaboration with Sharjah Blood Transfusion and Research Centre and
the Government of United Arab Emirates (UAE), is planning to organize the
WHO Global Forum for Blood Safety:
Patient Blood Management
on 13-14 March 2011 in Dubai, UAE. The aim of this forum is to provide a mechanism
for information exchange, fostering collaboration, involving international partners in
the implementation of resolution WHA63.R12 on availability, safety and quality of
blood products, particularly on patient blood management system.
Western Australian PBM ProjectRationale for patient blood management
There are compelling reasons for implementing
Patient blood management:
• Blood supply pressures
• Cost of blood
• Transfusion practice variability
• Transfusion safety and effectiveness
© Axel Hofmann AIC Graz 09-2010
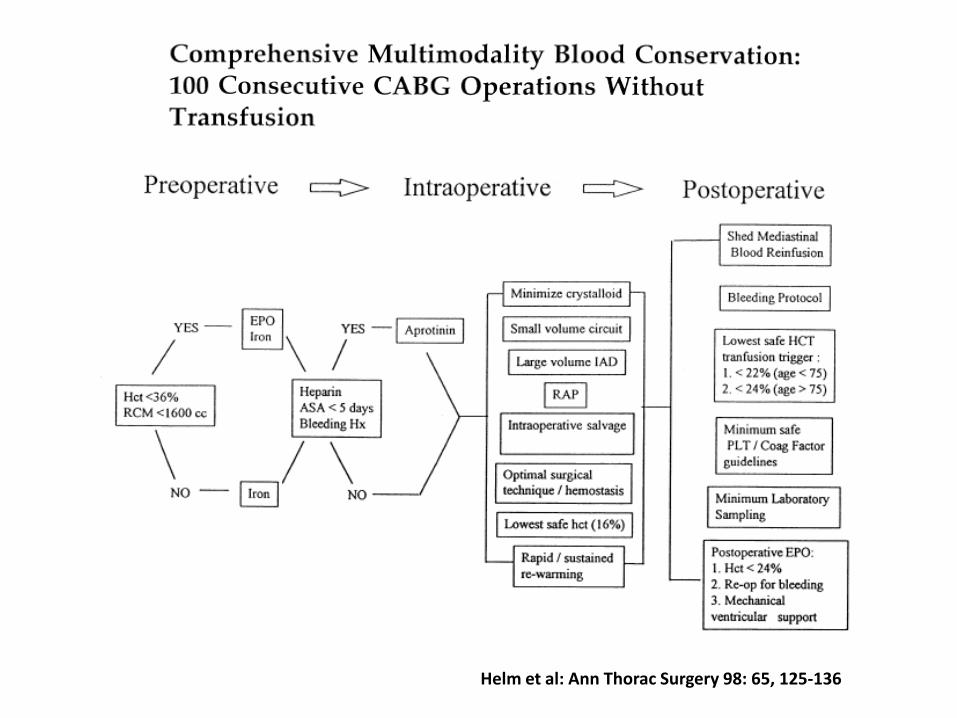
Helm et al: Ann Thorac Surgery 98: 65, 125-136
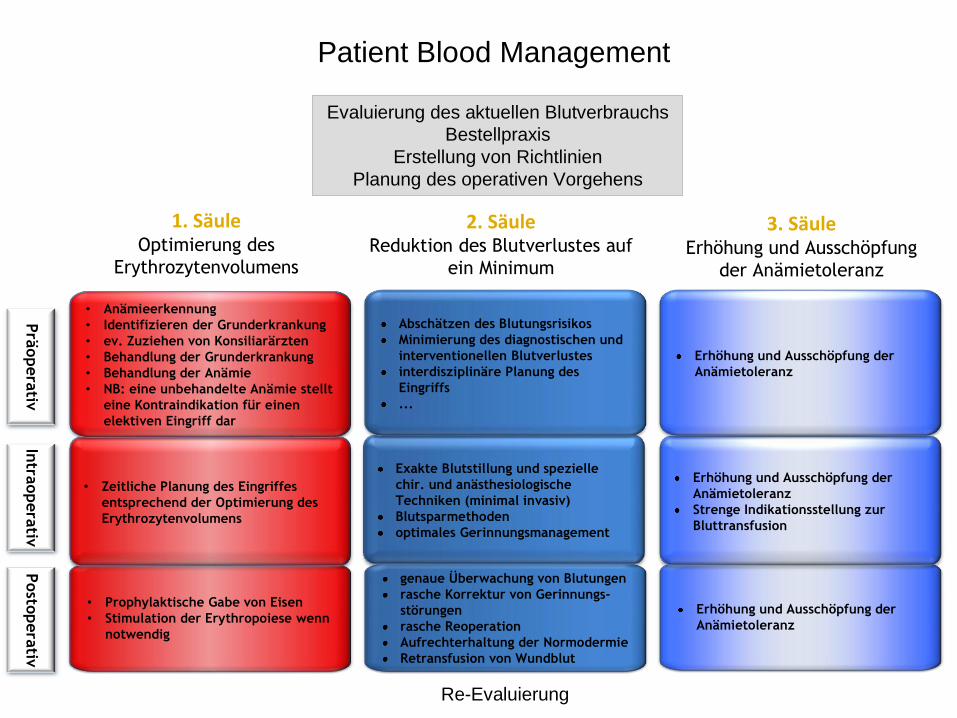
Prä
opera
tiv
• Prophylaktische Gabe von Eisen
• Stimulation der Erythropoiese wenn
notwendig
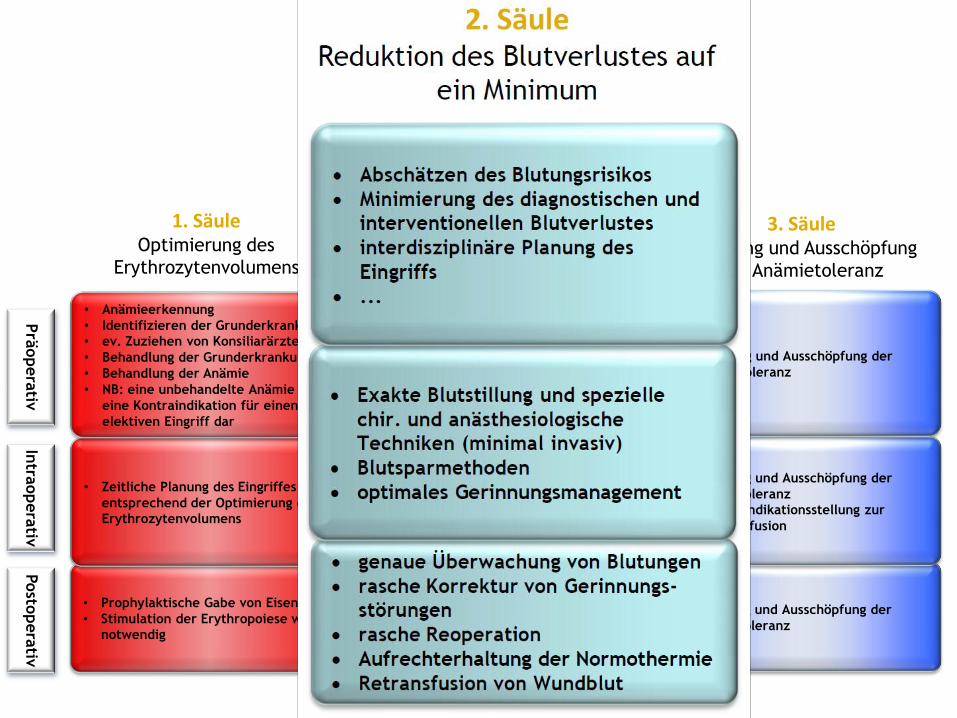
genaue Überwachung von Blutungen
rasche Korrektur von Gerinnungs-
störungen
rasche Reoperation
Aufrechterhaltung der Normodermie
Retransfusion von Wundblut
Erhöhung und Ausschöpfung der
Anämietoleranz
• Zeitliche Planung des Eingriffes
entsprechend der Optimierung des
Erythrozytenvolumens
Exakte Blutstillung und spezielle
chir. und anästhesiologische
Techniken (minimal invasiv)
Blutsparmethoden
optimales Gerinnungsmanagement
Erhöhung und Ausschöpfung der
Anämietoleranz
Strenge Indikationsstellung zur
Bluttransfusion
• Anämieerkennung
• Identifizieren der Grunderkrankung
• ev. Zuziehen von Konsiliarärzten
• Behandlung der Grunderkrankung
• Behandlung der Anämie
• NB: eine unbehandelte Anämie stellt
eine Kontraindikation für einen
elektiven Eingriff dar
Abschätzen des Blutungsrisikos
Minimierung des diagnostischen und
interventionellen Blutverlustes
interdisziplinäre Planung des
Eingriffs
...
Erhöhung und Ausschöpfung der
Anämietoleranz
Intra
opera
tivPosto
pera
tiv
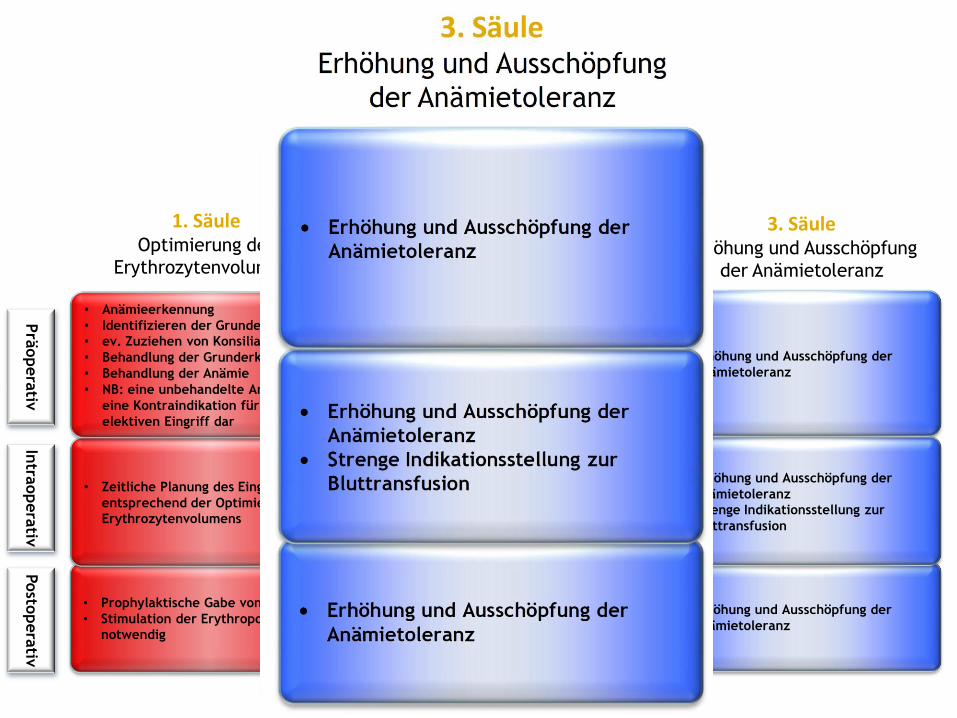
2. SäuleReduktion des Blutverlustes auf
ein Minimum
3. SäuleErhöhung und Ausschöpfung
der Anämietoleranz
1. SäuleOptimierung des
Erythrozytenvolumens
Evaluierung des aktuellen Blutverbrauchs
Bestellpraxis
Erstellung von Richtlinien
Planung des operativen Vorgehens
Re-Evaluierung
Patient Blood Management
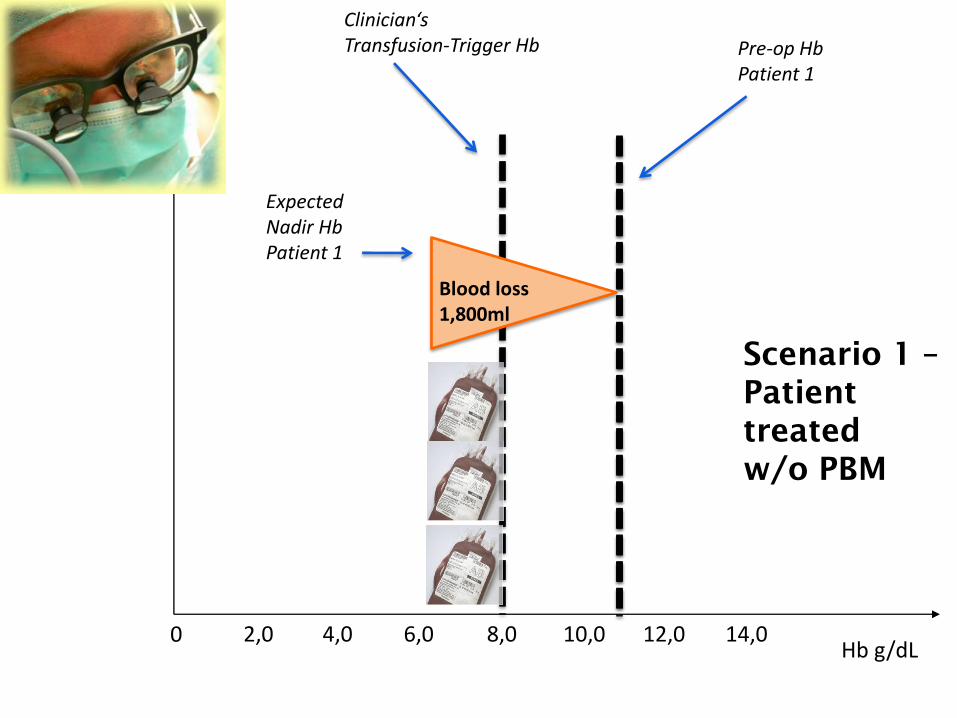
Hb g/dL0 4,0 6,0 8,0 10,0 12,0 14,02,0
Clinician‘sTransfusion-Trigger Hb Pre-op Hb
Patient 1
ExpectedNadir HbPatient 1
Blood loss1,800ml
Scenario 1 –
Patient
treated
w/o PBM
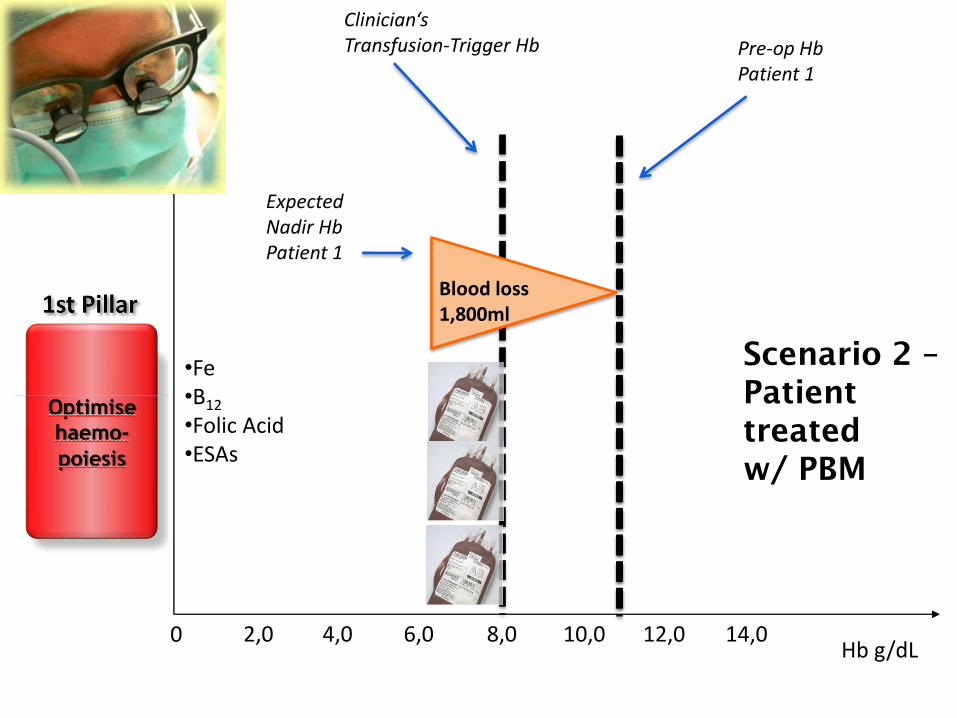
Hb g/dL0 4,0 6,0 8,0 10,0 12,0 14,02,0
ExpectedNadir HbPatient 1
Pre-op HbPatient 1
Blood loss1,800ml
•Fe•B12
•Folic Acid•ESAs
Clinician‘sTransfusion-Trigger Hb
Scenario 2 –
Patient
treated
w/ PBM

Hb g/dL0 4,0 6,0 8,0 10,0 12,0 14,02,0
© Axel Hofmann Vienna Vifor 09-2010
ExpectedNadir HbPatient 1
Pre-op HbPatient 1
Blood loss1,800ml
•Meticulous surgical hemostasis,•Topical hemostatic agents•Systemic hemostatic agents•Anesthesiological
techniques•Normothermia•Induced hypotension•etc.
Blood loss1,000ml
Clinician‘sTransfusion-Trigger Hb
Scenario 2 –
Patient
treated
w/ PBM
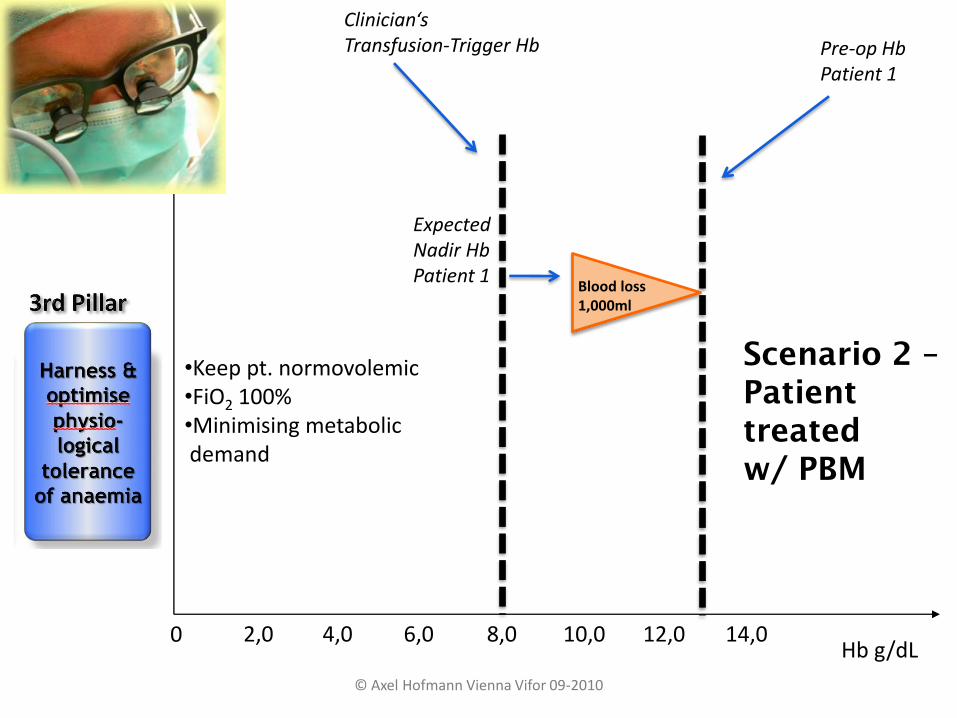
Hb g/dL0 4,0 6,0 8,0 10,0 12,0 14,02,0
© Axel Hofmann Vienna Vifor 09-2010
ExpectedNadir HbPatient 1
Pre-op HbPatient 1
•Keep pt. normovolemic•FiO2 100%•Minimising metabolicdemand
Blood loss1,000ml
Clinician‘sTransfusion-Trigger Hb
Scenario 2 –
Patient
treated
w/ PBM
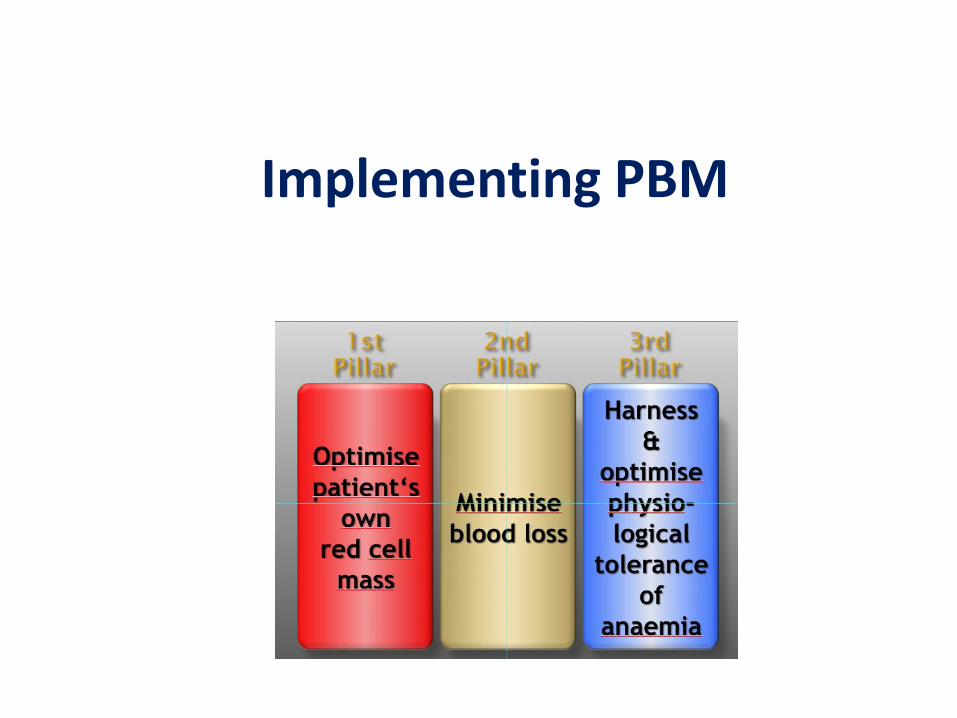
Implementing PBM
Predictors of Transfusion
• Type of surgery/surgeon
• Baseline hemoglobin and RBC mass
• Actual blood loss
• Co-morbidities
• Tolerable blood loss and transfusion trigger
(individual)

ESTIMATED AND CALCULATED BLOOD LOSS IN DIFFERENT TYPES OF SURGERY
Hip Knee Spine General CAGB Urologic
Predictors of Transfusion
• Type of surgery/surgeon
• Baseline hemoglobin and RBC mass
• Actual blood loss
• Co-morbidities
• Tolerable blood loss and transfusion trigger
(individual)
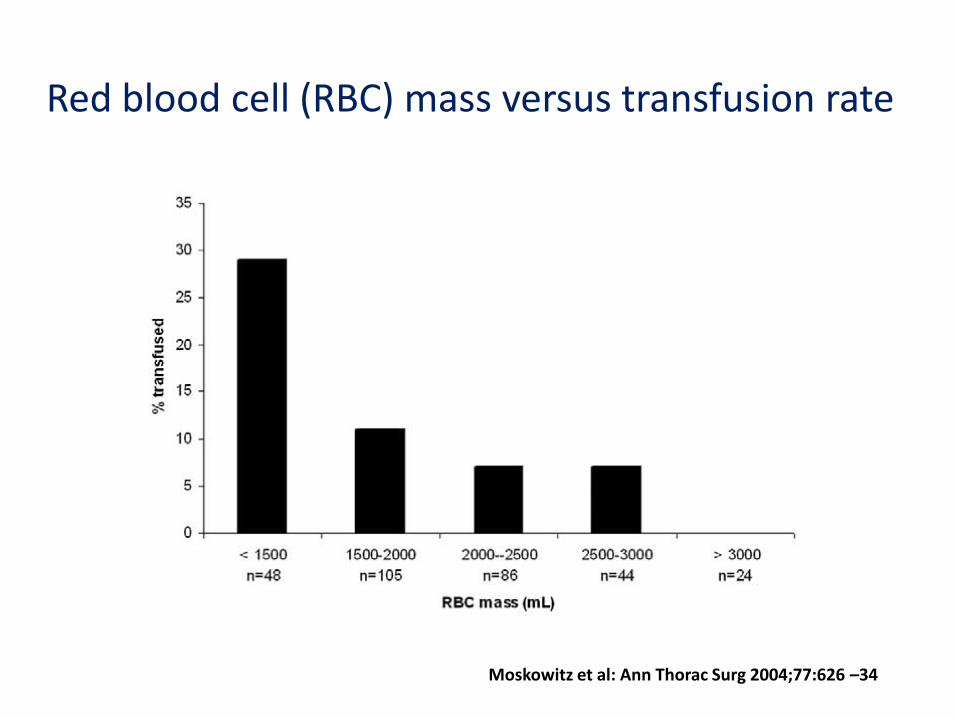
Red blood cell (RBC) mass versus transfusion rate
Moskowitz et al: Ann Thorac Surg 2004;77:626 –34
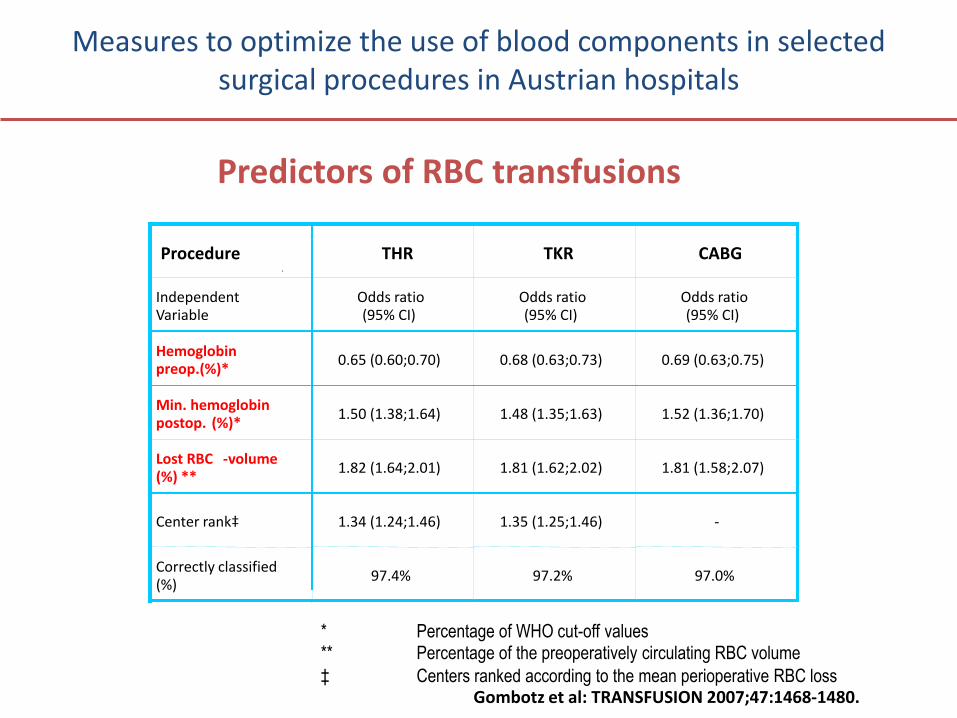
Measures to optimize the use of blood components in selected surgical procedures in Austrian hospitals
Predictors of RBC transfusions
Procedure THR TKR CABG
IndependentVariable
Odds ratio(95% CI)
Odds ratio(95% CI)
Odds ratio(95% CI)
Hemoglobin preop.(%)*
0.65 (0.60;0.70) 0.68 (0.63;0.73) 0.69 (0.63;0.75)
Min. hemoglobin postop. (%)*
1.50 (1.38;1.64) 1.48 (1.35;1.63) 1.52 (1.36;1.70)
Lost RBC -volume (%) **
1.82 (1.64;2.01) 1.81 (1.62;2.02) 1.81 (1.58;2.07)
Center rank‡ 1.34 (1.24;1.46) 1.35 (1.25;1.46) -
Correctly classified (%)
97.4% 97.2% 97.0%
* Percentage of WHO cut-off values** Percentage of the preoperatively circulating RBC volume
‡ Centers ranked according to the mean perioperative RBC lossGombotz et al: TRANSFUSION 2007;47:1468-1480.
Predictors of Transfusion
• Type of surgery/surgeon
• Baseline hemoglobin and RBC mass
• Actual blood loss
• Co-morbidities
• Tolerable blood loss ând transfusion trigger
(individual)
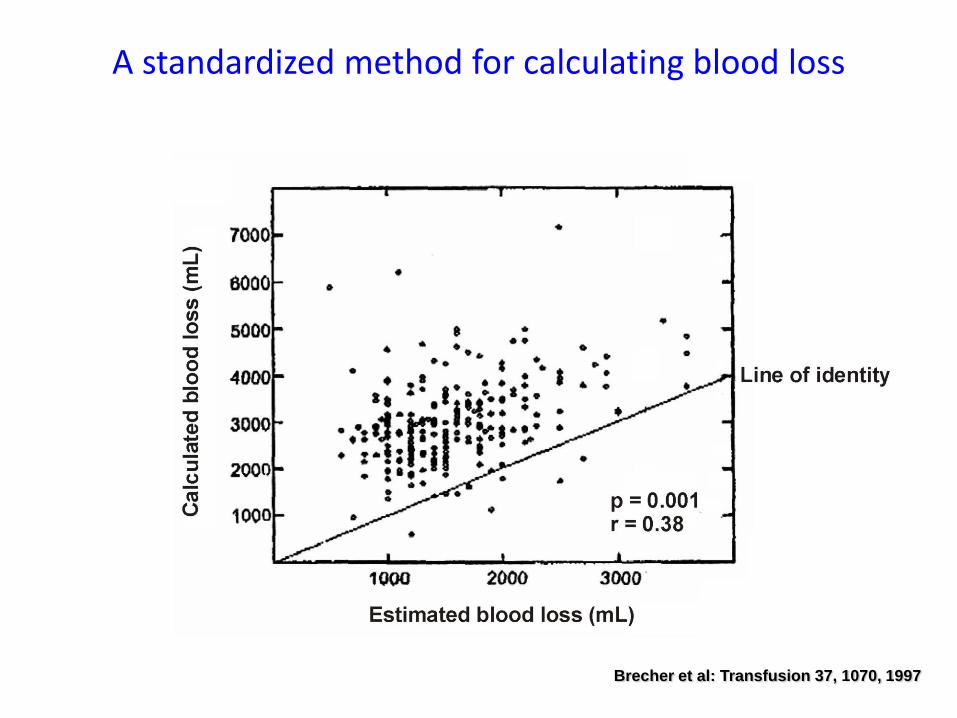
A standardized method for calculating blood loss
Brecher et al: Transfusion 37, 1070, 1997
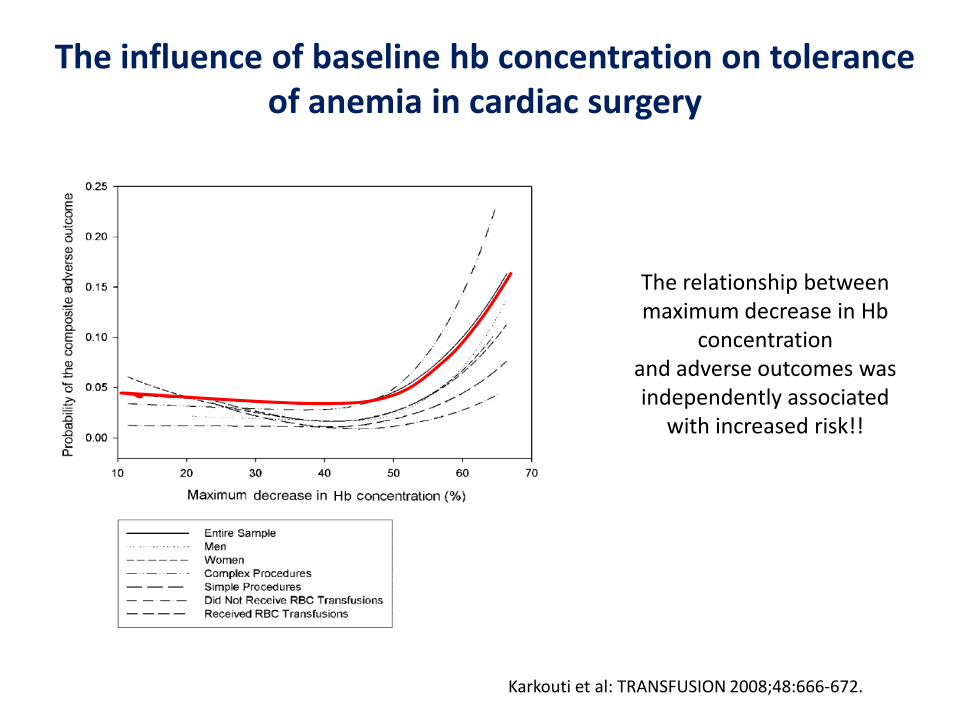
The influence of baseline hb concentration on toleranceof anemia in cardiac surgery
Karkouti et al: TRANSFUSION 2008;48:666-672.
The relationship between maximum decrease in Hb
concentrationand adverse outcomes was independently associated
with increased risk!!
Predictors of Transfusion
• Type of surgery/surgeon
• Baseline hemoglobin and RBC mass
• Actual blood loss
• Co-morbidities
• Tolerable blood loss and transfusion trigger
(individual)

Comorbidities of Anemic Patients
Beattie et al. Anesthesiology 2009; 110:574–81

Risk for perioperative myocardial
infarction and mortality in
patients undergoing hip or knee
arthroplasty: the role of anemia
Mantilla et al: TRANSFUSION 51, 82-91 :2011
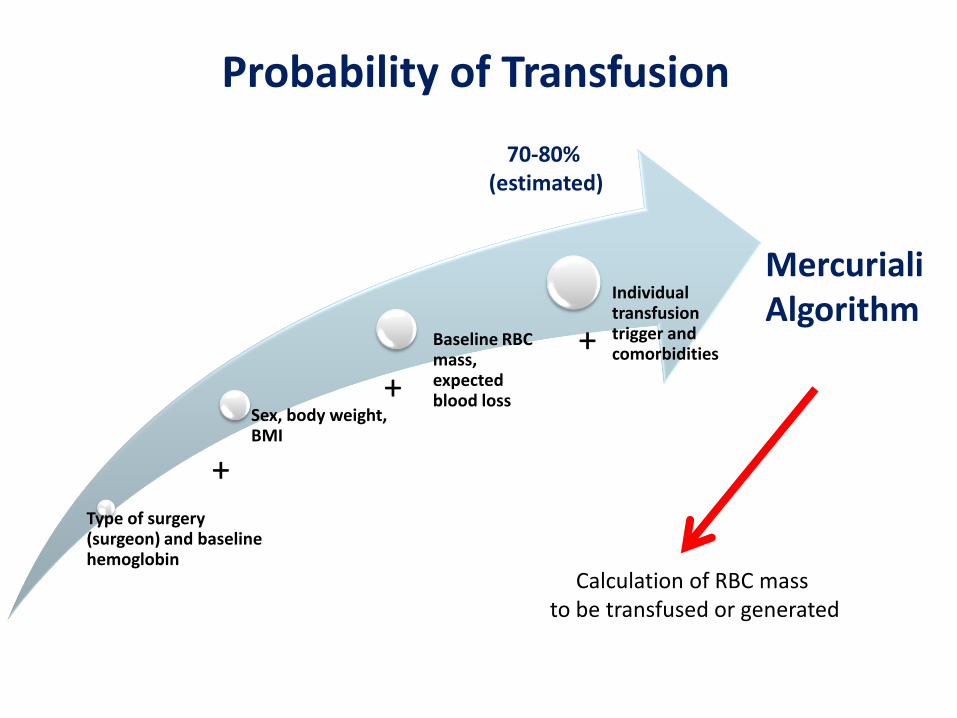
Type of surgery (surgeon) and baseline hemoglobin
Sex, body weight, BMI
Baseline RBC mass, expected blood loss
Individual transfusion trigger and comorbidities
Probability of Transfusion
70-80% (estimated)
+
+
+
MercurialiAlgorithm
Calculation of RBC mass to be transfused or generated
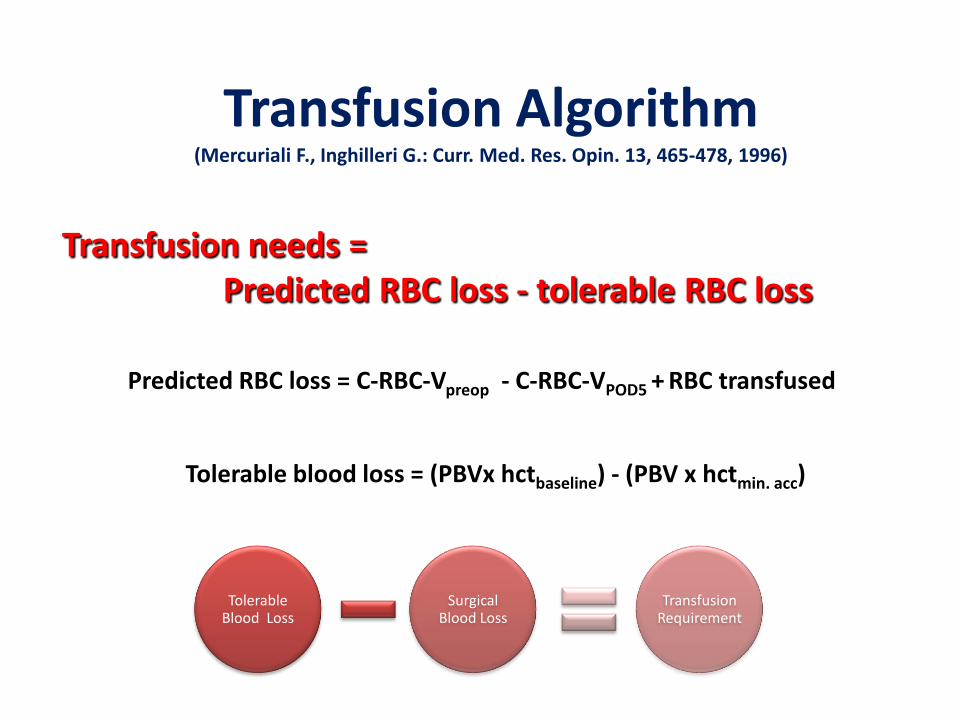
Transfusion Algorithm(Mercuriali F., Inghilleri G.: Curr. Med. Res. Opin. 13, 465-478, 1996)
Transfusion needs = Predicted RBC loss - tolerable RBC loss
Predicted RBC loss = C-RBC-Vpreop - C-RBC-VPOD5 + RBC transfused
Tolerable blood loss = (PBVx hctbaseline) - (PBV x hctmin. acc)
Tolerable Blood Loss
SurgicalBlood Loss
Transfusion Requirement
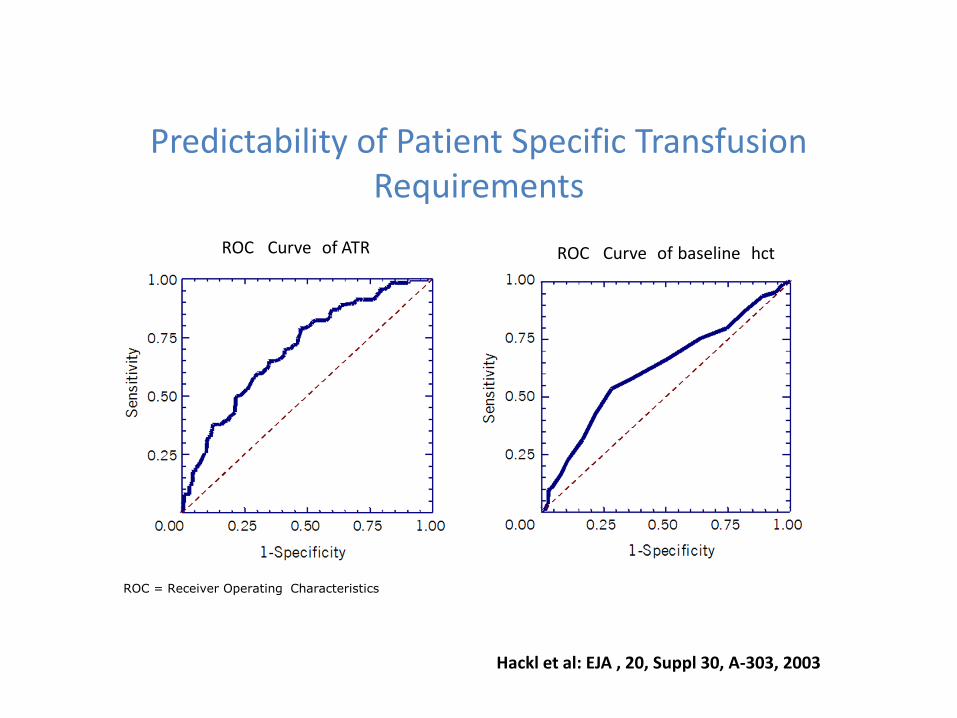
Predictability of Patient Specific Transfusion Requirements
ROC Curve of ATR ROC Curve of baseline hct
ROC = Receiver Operating Characteristics
Hackl et al: EJA , 20, Suppl 30, A-303, 2003
Components of PBM
Evaluation of the actual blood usage (data management)
Optimising blood ordering schedules
Increasing tolerance of anemia
3 pillar strategy
– Optimising preoperative red cell mass
– Minimising perioperative blood loss
– Reducing transfusion trigger
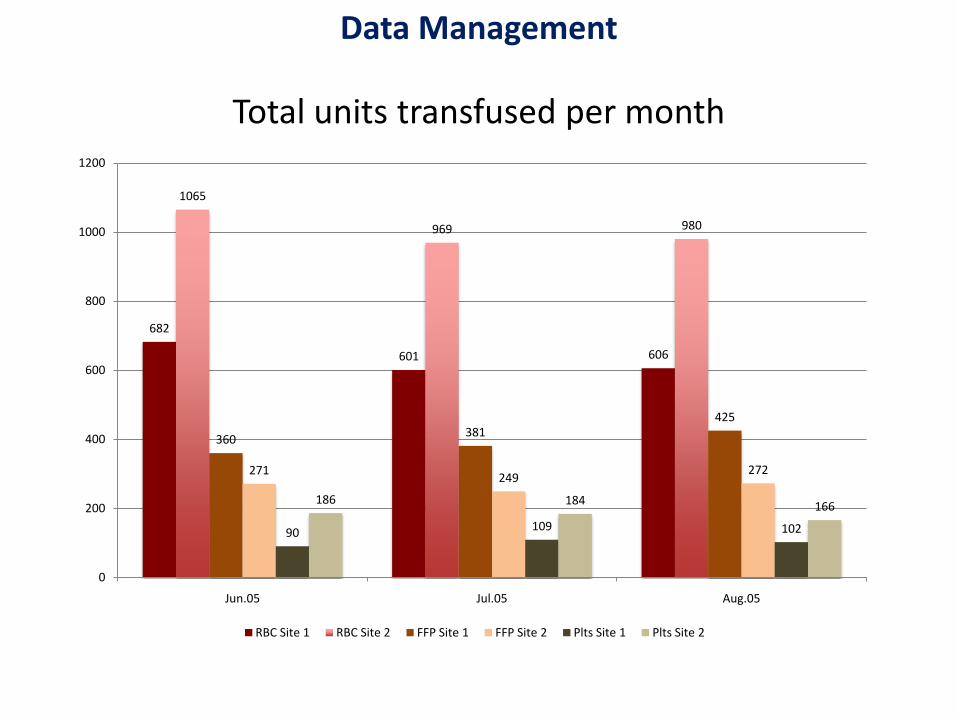
Total units transfused per month
682
601 606
1065
969 980
360381
425
271249
272
90 109 102
186 184 166
0
200
400
600
800
1000
1200
Jun.05 Jul.05 Aug.05
RBC Site 1 RBC Site 2 FFP Site 1 FFP Site 2 Plts Site 1 Plts Site 2
Data Management
Components of PBM
Evaluation of the actual blood usage (data management)
Optimising blood ordering schedules
Increasing tolerance of anemia
3 pillar strategy
– Optimising preoperative red cell mass
– Minimising perioperative blood loss
– Reducing transfusion trigger
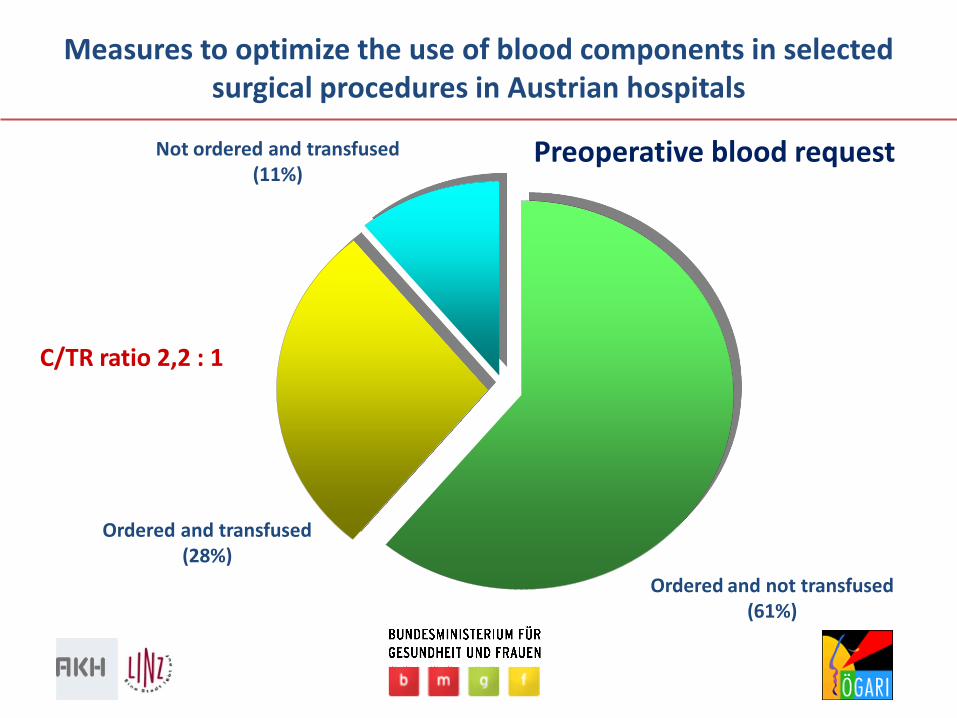
Measures to optimize the use of blood components in selected surgical procedures in Austrian hospitals
Ordered and not transfused(61%)
Ordered and transfused(28%)
Not ordered and transfused(11%)
Preoperative blood request
C/TR ratio 2,2 : 1
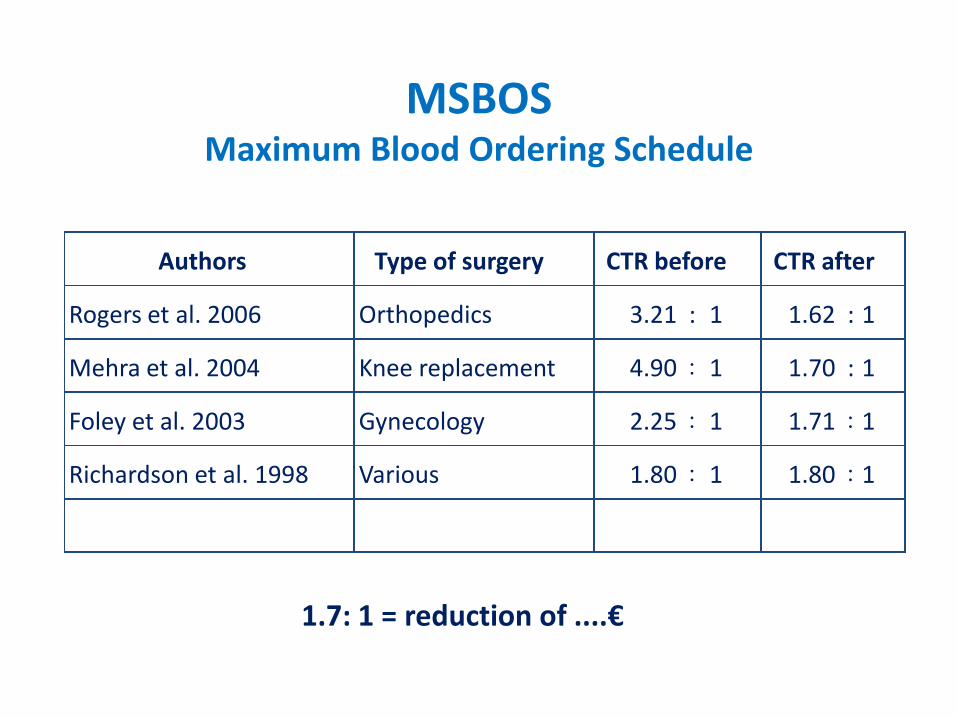
MSBOSMaximum Blood Ordering Schedule
Authors Type of surgery CTR before CTR after
Rogers et al. 2006 Orthopedics 3.21 : 1 1.62 : 1
Mehra et al. 2004 Knee replacement 4.90 : 1 1.70 : 1
Foley et al. 2003 Gynecology 2.25 : 1 1.71 : 1
Richardson et al. 1998 Various 1.80 : 1 1.80 : 1
1.7: 1 = reduction of ....€
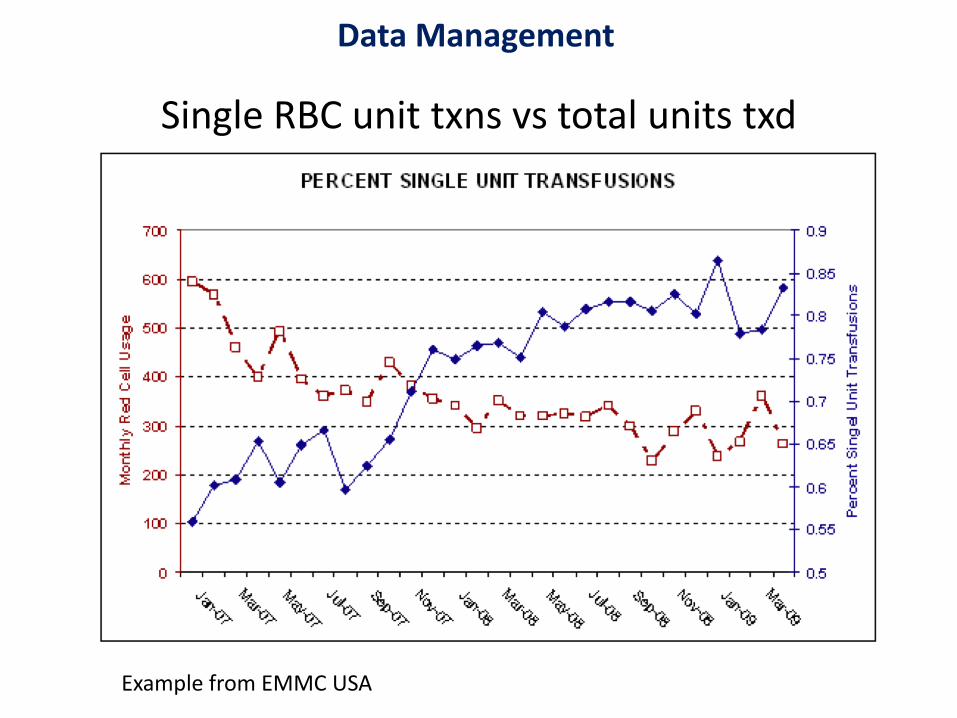
Single RBC unit txns vs total units txd
Example from EMMC USA
Data Management
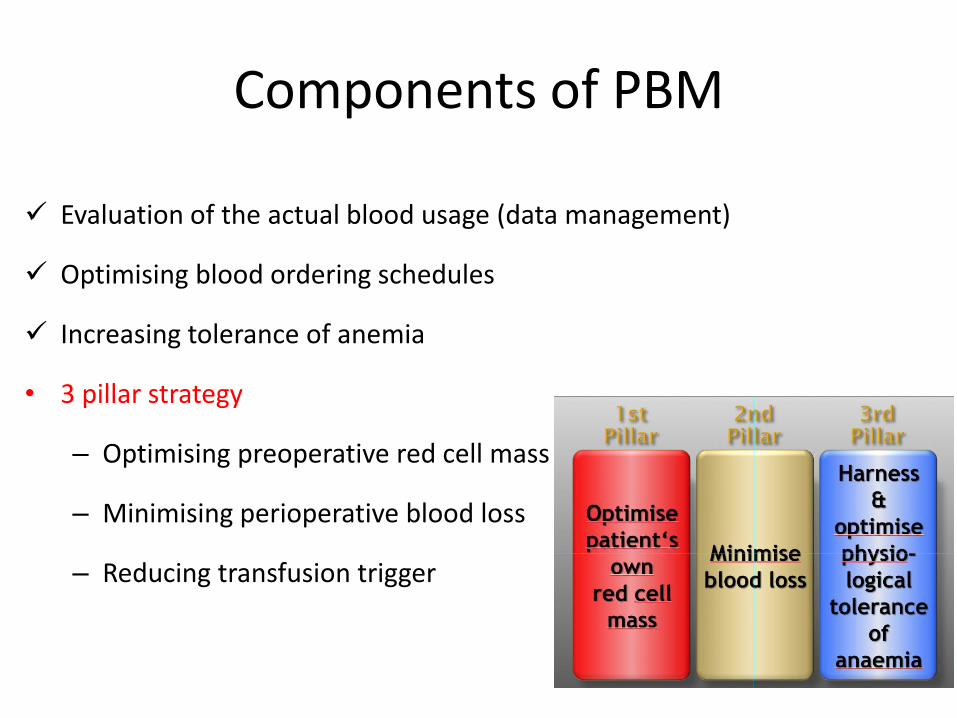
Components of PBM
Evaluation of the actual blood usage (data management)
Optimising blood ordering schedules
Increasing tolerance of anemia
• 3 pillar strategy
– Optimising preoperative red cell mass
– Minimising perioperative blood loss
– Reducing transfusion trigger
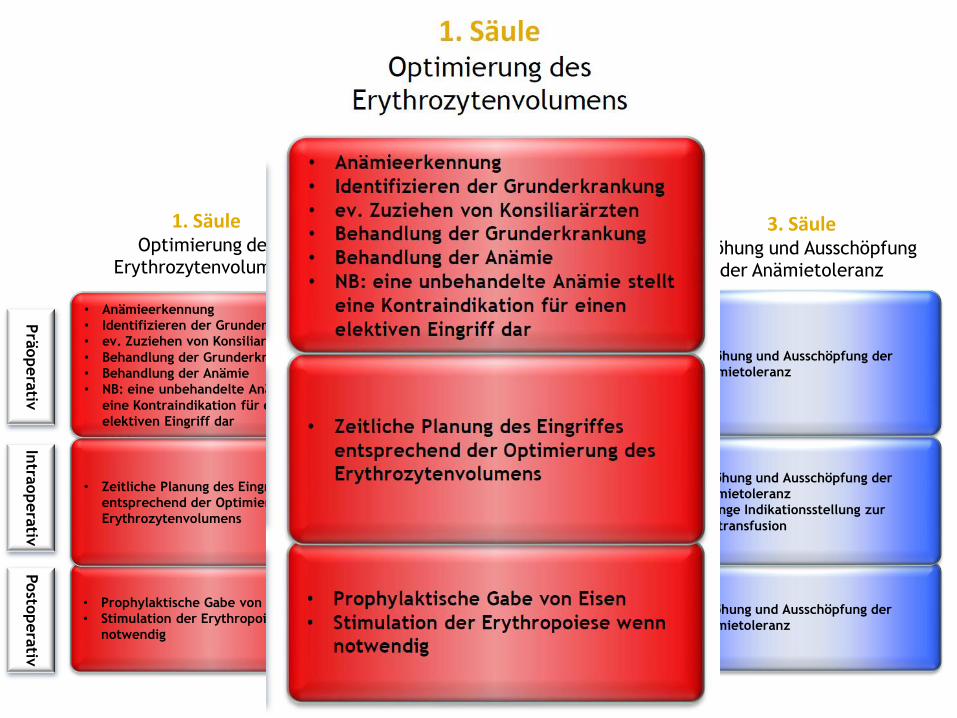
Prä
opera
tiv
• Prophylaktische Gabe von Eisen
• Stimulation der Erythropoiese wenn
notwendig
genaue Überwachung von Blutungen
rasche Korrektur von Gerinnungs-
störungen
rasche Reoperation
Aufrechterhaltung der Normodermie
Retransfusion von Wundblut
Erhöhung und Ausschöpfung der
Anämietoleranz
• Zeitliche Planung des Eingriffes
entsprechend der Optimierung des
Erythrozytenvolumens
Exakte Blutstillung und spezielle
chir. und anästhesiologische
Techniken (minimal invasiv)
Blutsparmethoden
optimales Gerinnungsmanagement
Erhöhung und Ausschöpfung der
Anämietoleranz
Strenge Indikationsstellung zur
Bluttransfusion
• Anämieerkennung
• Identifizieren der Grunderkrankung
• ev. Zuziehen von Konsiliarärzten
• Behandlung der Grunderkrankung
• Behandlung der Anämie
• NB: eine unbehandelte Anämie stellt
eine Kontraindikation für einen
elektiven Eingriff dar
Abschätzen des Blutungsrisikos
Minimierung des diagnostischen und
interventionellen Blutverlustes
interdisziplinäre Planung des
Eingriffs
...
Erhöhung und Ausschöpfung der
Anämietoleranz
Intra
opera
tivPosto
pera
tiv
2. SäuleReduktion des Blutverlustes auf
ein Minimum
3. SäuleErhöhung und Ausschöpfung
der Anämietoleranz
1. SäuleOptimierung des
Erythrozytenvolumens
Evaluierung des aktuellen Blutverbrauchs
Bestellpraxis
Erstellung von Richtlinien
Planung des operativen Vorgehens
Re-Evaluierung
Patient Blood Management
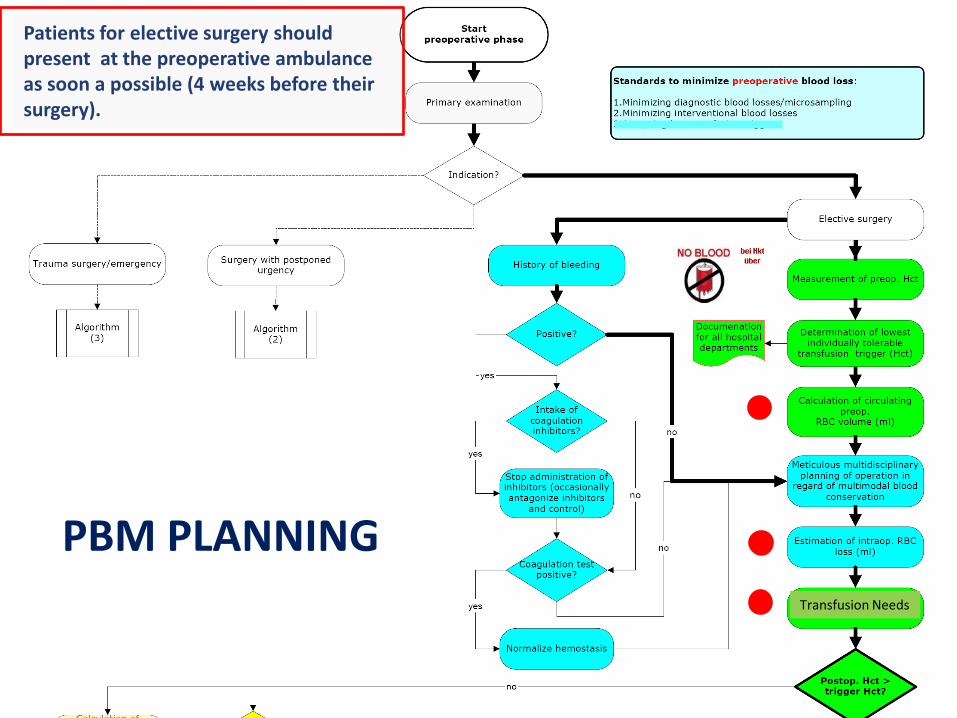
Transfusion Needs
Patients for elective surgery should present at the preoperative ambulance as soon a possible (4 weeks before their surgery).
PBM PLANNING
Präop. Aufklärung AKH Linz
"Sollten Sie unter Anämie leiden, weisen wir Sie darauf hin,
dass eine präoperative Anämiebehandlung diverse Risiken,
die mit der Operation verbunden sind (z.B erhöhte
Transfusionsrate, erhöhte Infektionsrate und Infarktrate und
damit verbunden ein längerer Krankenhausaufenthalt),
wesentlich reduzieren würden. Aus diesem Grund empfehlen
wir bei allen elektiven, also nicht ganz dringlichen Eingriffen
eine entsprechende Behandlung."

Hgb < 120 g/L for femalesHgb < 130 g/L for males
ferritin < 30 mcg/L and/or TSAT < 15-
20%
ferritin 30-70 mcg/Land/or TSAT > 20%
Normal
Ferritin? TSAT?
Serum creatinineGFR
Anemia of chronic disease
Low Vitamin B12
and/or folic acid
ferritin > 70 mcg/Land/or TSAT > 20%
NormalChronic kidney disease (CKD)
Low
R/O iron deficiency
Inflammation/ chronic disease
Iron deficiency Referral to
gastroenterologist to R/O malignancy
Folic acid and/orVitamin B12 therapyESA TherapyIron Therapy
1 – Oral iron in divided doses2 – IV iron in divided doses
if patient cannot tolerate oral iron,intestinal absorption problems, or
short timeline
Refer to nephrologist
No response
No action required
Evaluation necessary
Goodnough et al: Nata guidelines, BJA in print
Empfehlungen II
Circulation 2005;112;1681-1683
Prä
opera
tiv
• Prophylaktische Gabe von Eisen
• Stimulation der Erythropoiese wenn
notwendig
genaue Überwachung von Blutungen
rasche Korrektur von Gerinnungs-
störungen
rasche Reoperation
Aufrechterhaltung der Normothermie
Retransfusion von Wundblut
Erhöhung und Ausschöpfung der
Anämietoleranz
• Zeitliche Planung des Eingriffes
entsprechend der Optimierung des
Erythrozytenvolumens
Exakte Blutstillung und spezielle
chir. und anästhesiologische
Techniken (minimal invasiv)
Blutsparmethoden
optimales Gerinnungsmanagement
Erhöhung und Ausschöpfung der
Anämietoleranz
Strenge Indikationsstellung zur
Bluttransfusion
• Anämieerkennung
• Identifizieren der Grunderkrankung
• ev. Zuziehen von Konsiliarärzten
• Behandlung der Grunderkrankung
• Behandlung der Anämie
• NB: eine unbehandelte Anämie stellt
eine Kontraindikation für einen
elektiven Eingriff dar
Abschätzen des Blutungsrisikos
Minimierung des diagnostischen und
interventionellen Blutverlustes
interdisziplinäre Planung des
Eingriffs
...
Erhöhung und Ausschöpfung der
Anämietoleranz
Intra
opera
tivPosto
pera
tiv
2. SäuleReduktion des Blutverlustes auf
ein Minimum
3. SäuleErhöhung und Ausschöpfung
der Anämietoleranz
1. SäuleOptimierung des
Erythrozytenvolumens
Evaluierung des aktuellen Blutverbrauchs
Bestellpraxis
Erstellung von Richtlinien
Planung des operativen Vorgehens
Re-Evaluierung
Patient Blood Management
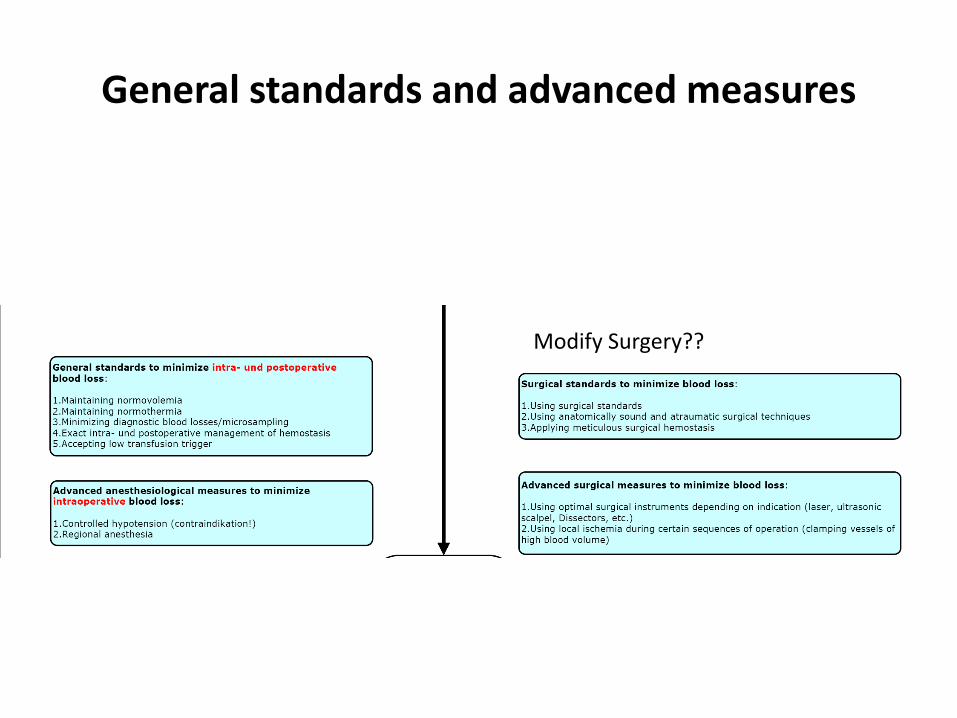
General standards and advanced measures
Modify Surgery??
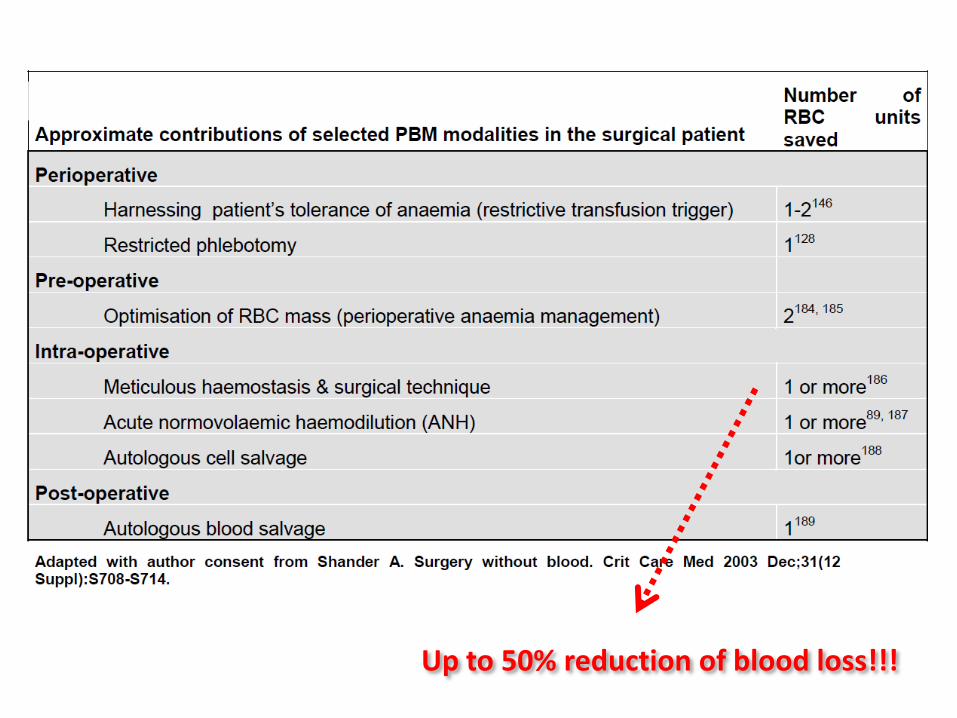
Up to 50% reduction of blood loss!!!
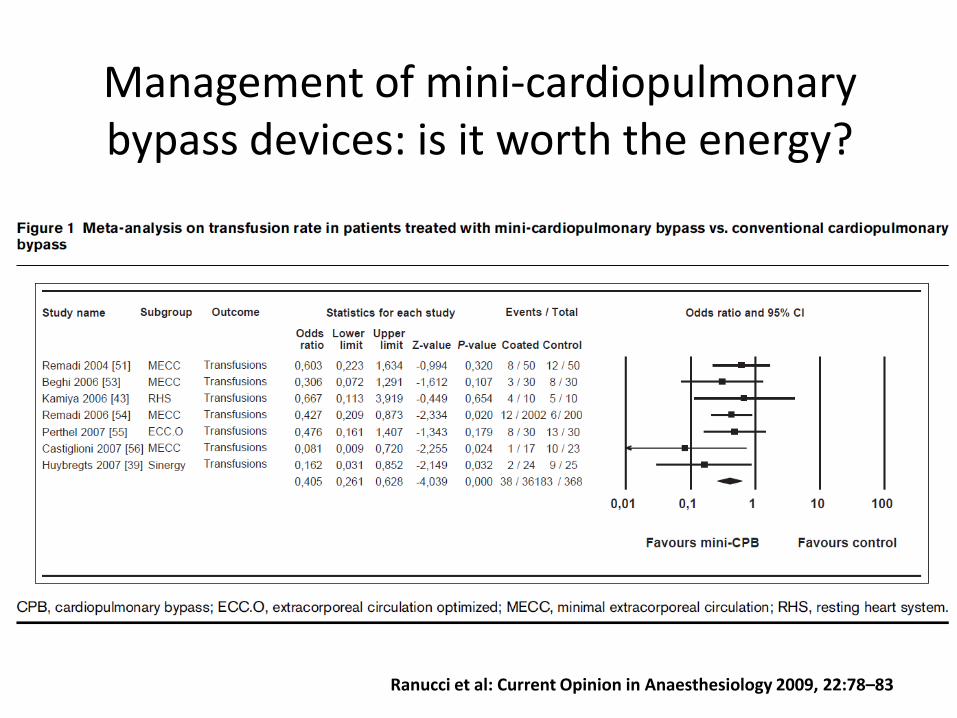
Management of mini-cardiopulmonary bypass devices: is it worth the energy?
Ranucci et al: Current Opinion in Anaesthesiology 2009, 22:78–83
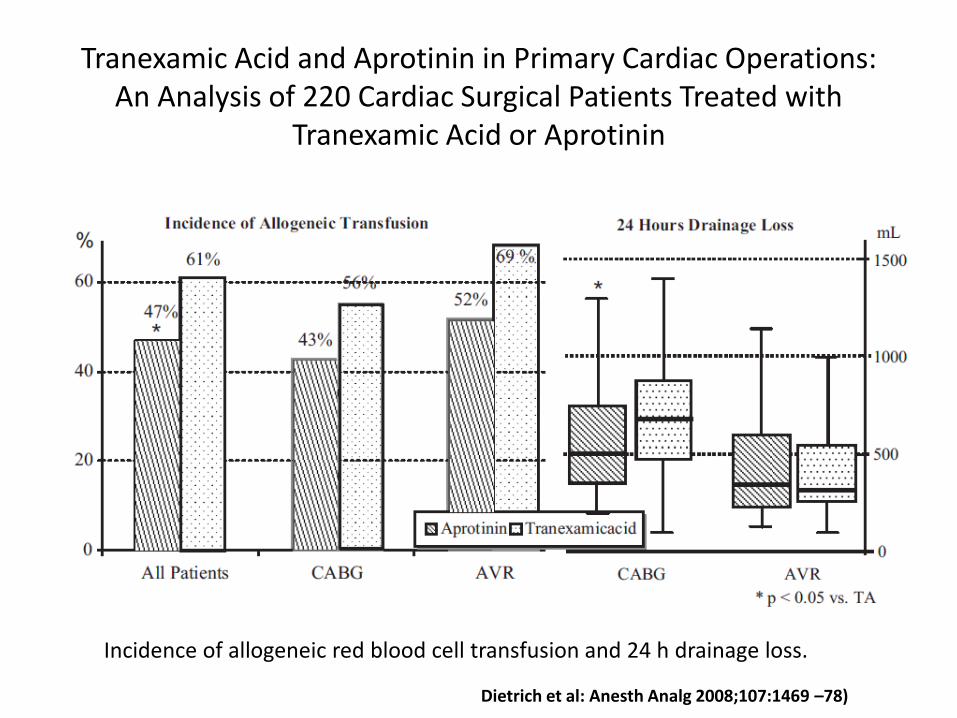
Tranexamic Acid and Aprotinin in Primary Cardiac Operations: An Analysis of 220 Cardiac Surgical Patients Treated with
Tranexamic Acid or Aprotinin
Incidence of allogeneic red blood cell transfusion and 24 h drainage loss.
Dietrich et al: Anesth Analg 2008;107:1469 –78)
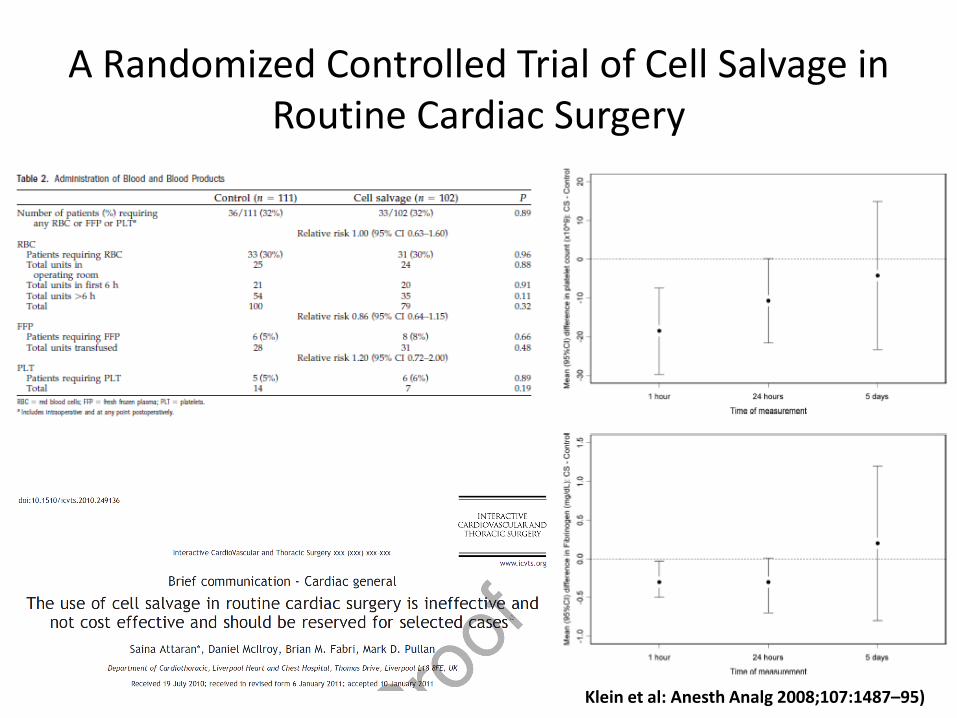
A Randomized Controlled Trial of Cell Salvage in Routine Cardiac Surgery
Klein et al: Anesth Analg 2008;107:1487–95)
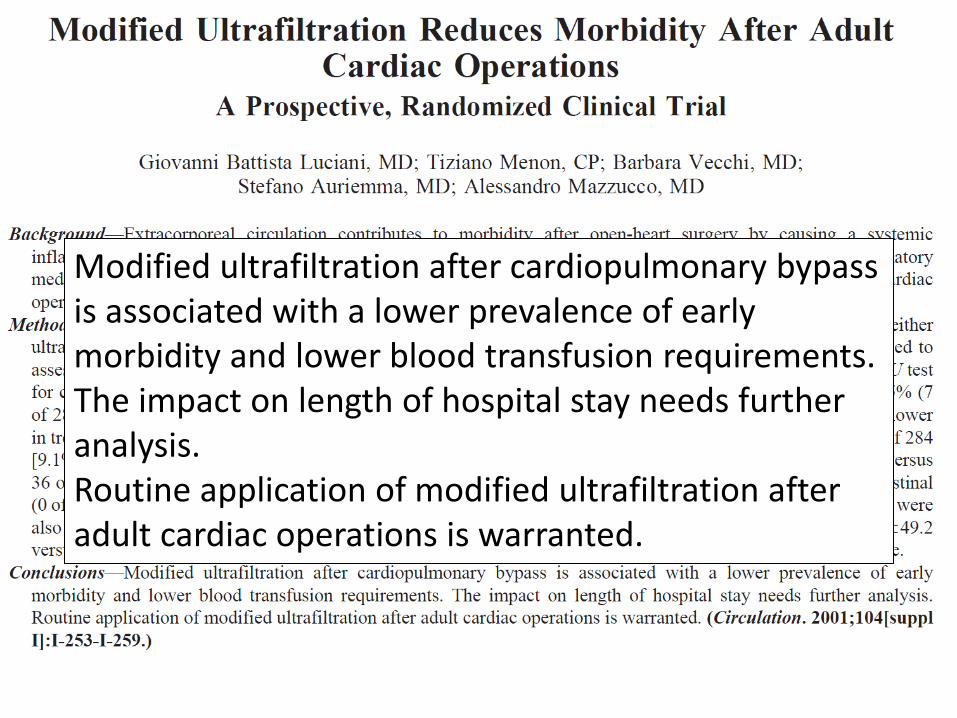
Modified ultrafiltration after cardiopulmonary bypass is associated with a lower prevalence of early morbidity and lower blood transfusion requirements. The impact on length of hospital stay needs further analysis.Routine application of modified ultrafiltration after adult cardiac operations is warranted.
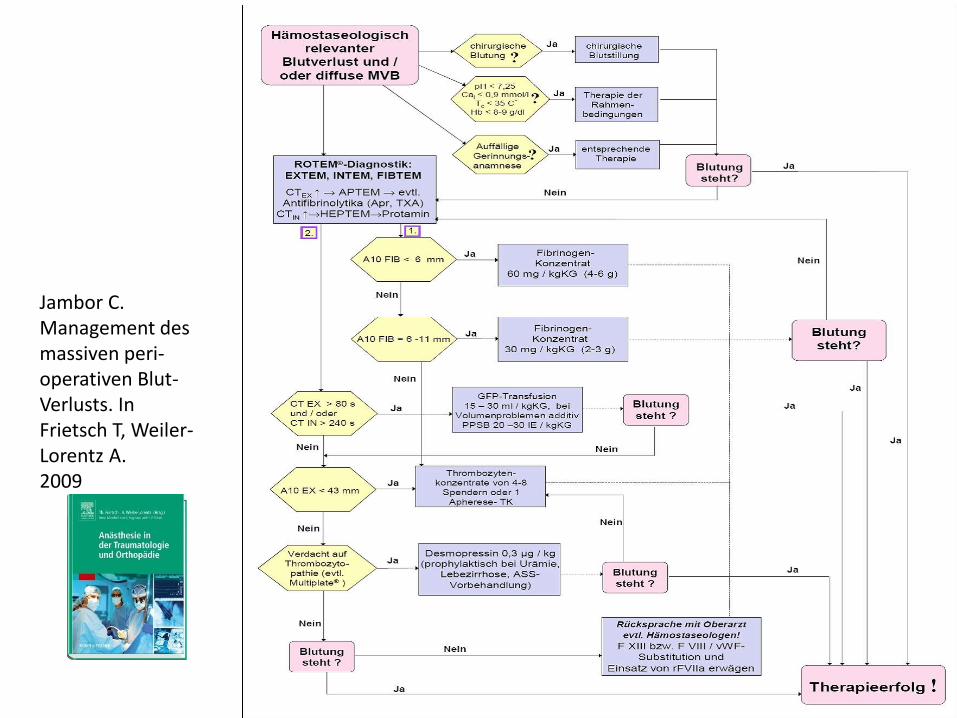
Rotem®
basierter Algorithmus
Jambor C.Management des massiven peri-operativen Blut-Verlusts. InFrietsch T, Weiler-Lorentz A.2009
Prä
opera
tiv
• Prophylaktische Gabe von Eisen
• Stimulation der Erythropoiese wenn
notwendig
genaue Überwachung von Blutungen
rasche Korrektur von Gerinnungs-
störungen
rasche Reoperation
Aufrechterhaltung der Normodermie
Retransfusion von Wundblut
Erhöhung und Ausschöpfung der
Anämietoleranz
• Zeitliche Planung des Eingriffes
entsprechend der Optimierung des
Erythrozytenvolumens
Exakte Blutstillung und spezielle
chir. und anästhesiologische
Techniken (minimal invasiv)
Blutsparmethoden
optimales Gerinnungsmanagement
Erhöhung und Ausschöpfung der
Anämietoleranz
Strenge Indikationsstellung zur
Bluttransfusion
• Anämieerkennung
• Identifizieren der Grunderkrankung
• ev. Zuziehen von Konsiliarärzten
• Behandlung der Grunderkrankung
• Behandlung der Anämie
• NB: eine unbehandelte Anämie stellt
eine Kontraindikation für einen
elektiven Eingriff dar
Abschätzen des Blutungsrisikos
Minimierung des diagnostischen und
interventionellen Blutverlustes
interdisziplinäre Planung des
Eingriffs
...
Erhöhung und Ausschöpfung der
Anämietoleranz
Intra
opera
tivPosto
pera
tiv
2. SäuleReduktion des Blutverlustes auf
ein Minimum
3. SäuleErhöhung und Ausschöpfung
der Anämietoleranz
1. SäuleOptimierung des
Erythrozytenvolumens
Evaluierung des aktuellen Blutverbrauchs
Bestellpraxis
Erstellung von Richtlinien
Planung des operativen Vorgehens
Re-Evaluierung
Patient Blood Management

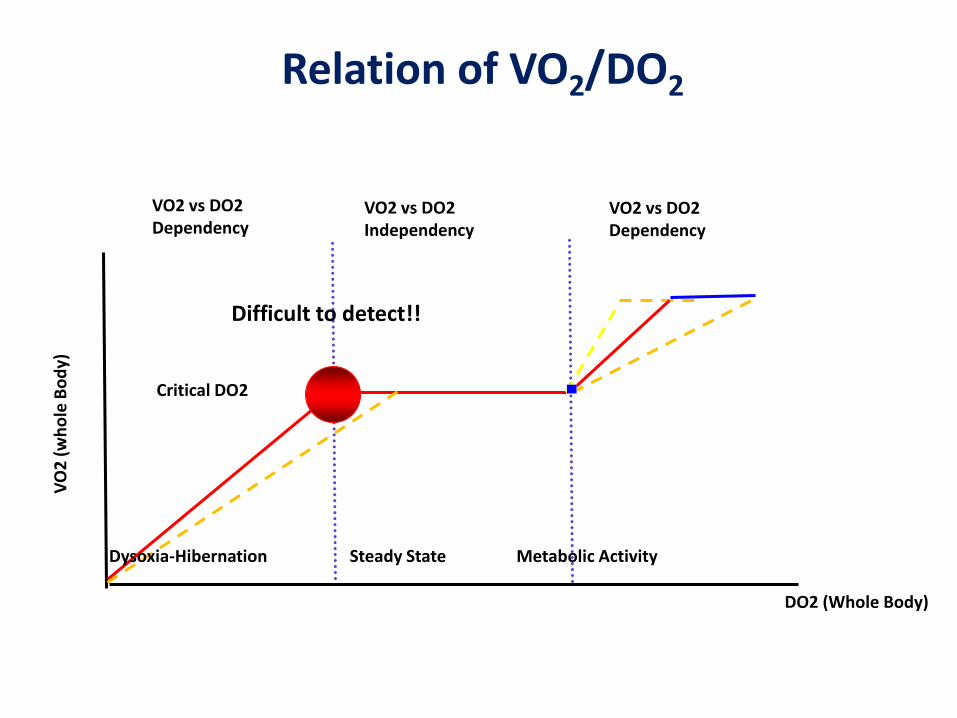
Relation of VO2/DO2
DO2 (Whole Body)
VO
2(w
ho
le B
od
y)
VO2 vs DO2Dependency
VO2 vs DO2Independency
VO2 vs DO2Dependency
Critical DO2
Dysoxia-Hibernation Steady State Metabolic Activity
Difficult to detect!!
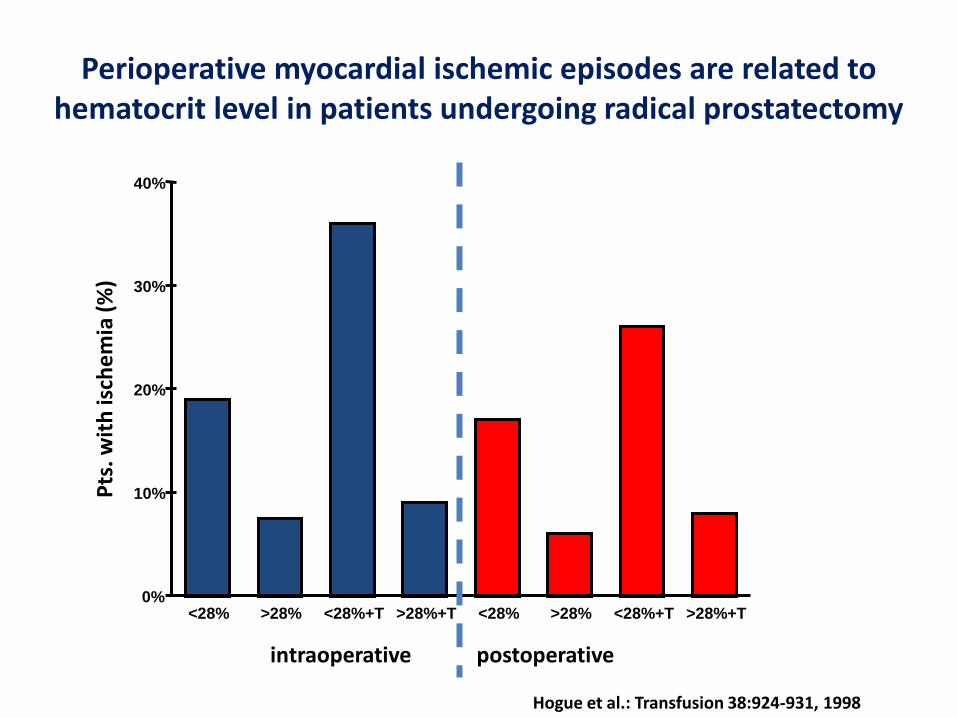
Perioperative myocardial ischemic episodes are related to hematocrit level in patients undergoing radical prostatectomy
<28% >28% <28%+T >28%+T <28% >28% <28%+T >28%+T0%
10%
20%
30%
40%
intraoperative postoperative
Pts
. wit
h is
che
mia
(%
)
Hogue et al.: Transfusion 38:924-931, 1998
^

Recommendations Regarding Indications for RBC Transfusion in the General Critically Ill Patient (1)
1. RBC transfusion is indicated for patients with evidence of hemorrhagic shock. (Level 1)
2. RBC transfusion may be indicated for patients with evidence of acute hemorrhage and hemodynamic instability or inadequate oxygen delivery. (Level 1)
3. A “restrictive” strategy of RBC transfusion (transfuse when Hb 7 g/dL) is as effective as a “liberal” transfusion strategy (transfusion when Hb 10 g/dL) in critically ill patients with hemodynamicallystable anemia, except possibly in patients with acute myocardial ischemia. (Level 1)
4. The use of only Hb level as a “trigger” for transfusion should be avoided. Decision for RBC transfusion should be based on an individual patient’s intravascular volume status, evidence of shock, duration and extent of anemia, and cardiopulmonary physiologic parameters. (Level 2)
5. In the absence of acute hemorrhage RBC, transfusion should be given as single units. (Level 2)
6. Consider transfusion if Hb 7g/dL in critically ill patients requiring mechanical ventilation (MV). There is no benefit of a “liberal”transfusion strategy (transfusion when Hb 10 g/dL) in critically ill patients requiring MV. (Level 2)
Napolitano et al: Crit Care Med 2009; 37:3124 –3157
Recommendations Regarding Indications for RBC Transfusion in the General Critically Ill Patient (2)
7. Consider transfusion if Hb 7 g/dL in resuscitated critically ill trauma patients. There is no benefit of a “liberal” transfusion strategy (transfusion when Hb 10 g/dL) in resuscitated critically ill trauma patients. (Level 2)
8. Consider transfusion if Hb 7 g/dL in critically ill patients with stable cardiac disease. There is no benefit of a “liberal” transfusion strategy (transfusion when Hb 10 g/dL) in critically ill patients with stable cardiac disease. (Level 2)
9. RBC transfusion should not be considered as an absolute method to improve tissue oxygen consumption in critically ill patients. (Level 2)
10. RBC transfusion may be beneficial in patients with acute coronary syndromes (ACS) who are anemic (Hb 8 g/dL) on hospital admission. (Level 3)
Napolitano et al: Crit Care Med 2009; 37:3124 –3157
Australia
© Axel Hofmann AIC Graz 09-2010© Axel Hofmann Vienna Vifor 09-2010
Transfusion thresholds and other strategies for guiding
allogeneic red blood cell transfusion
• Restrictive transfusion strategies reduced the risk of receiving a red
blood cell (RBC) transfusion by a relative 42%. This equates to an
average absolute risk reduction (ARR) of 40%.
• The volume of RBCs transfused was reduced on average by 0.93 units.
• However, heterogeneity between these trials was statistically
significant (p<0.00001) for these outcomes.
• Mortality, rates of cardiac events, morbidity, and length of hospital stay
were unaffected. Trials were of poor methodological quality.
Hill SR, et al: The Cochrane Library, Issue 4, 2003.
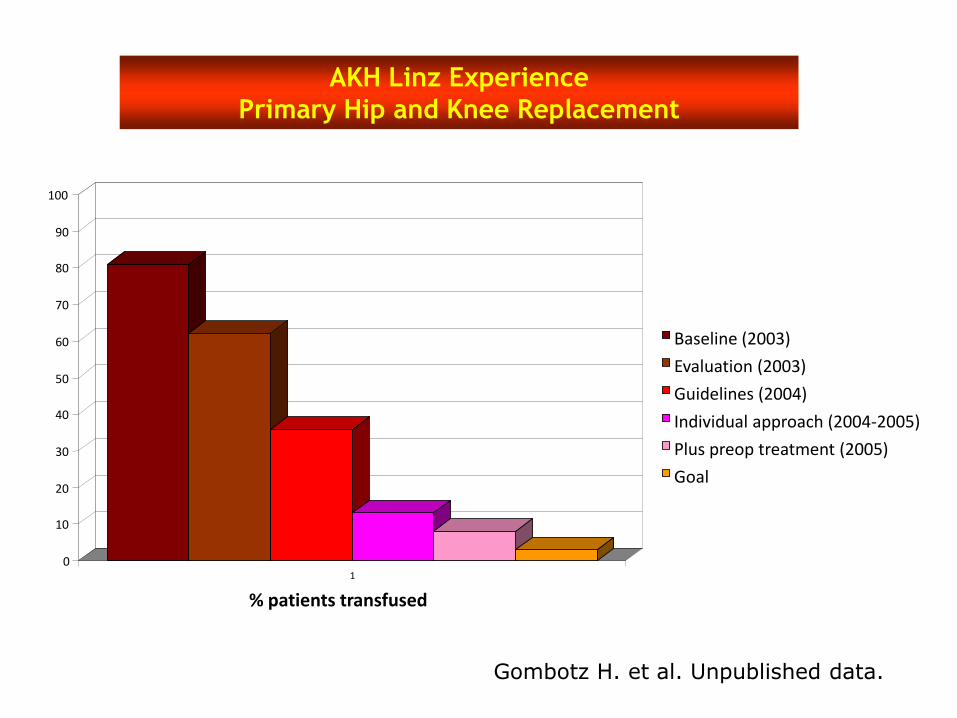
0
10
20
30
40
50
60
70
80
90
100
1
% patients transfused
Baseline (2003)
Evaluation (2003)
Guidelines (2004)
Individual approach (2004-2005)
Plus preop treatment (2005)
Goal
Gombotz H. et al. Unpublished data.
AKH Linz Experience
Primary Hip and Knee Replacement
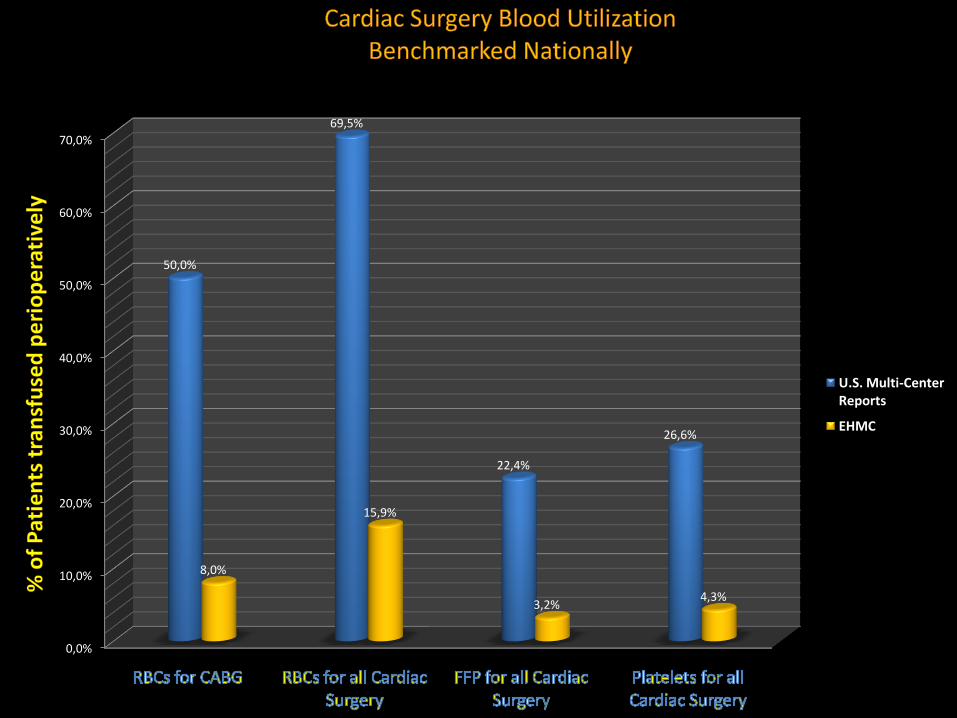
0,0%
10,0%
20,0%
30,0%
40,0%
50,0%
60,0%
70,0%
50,0%
69,5%
22,4%
26,6%
8,0%
15,9%
3,2%4,3%
U.S. Multi-CenterReports
EHMC
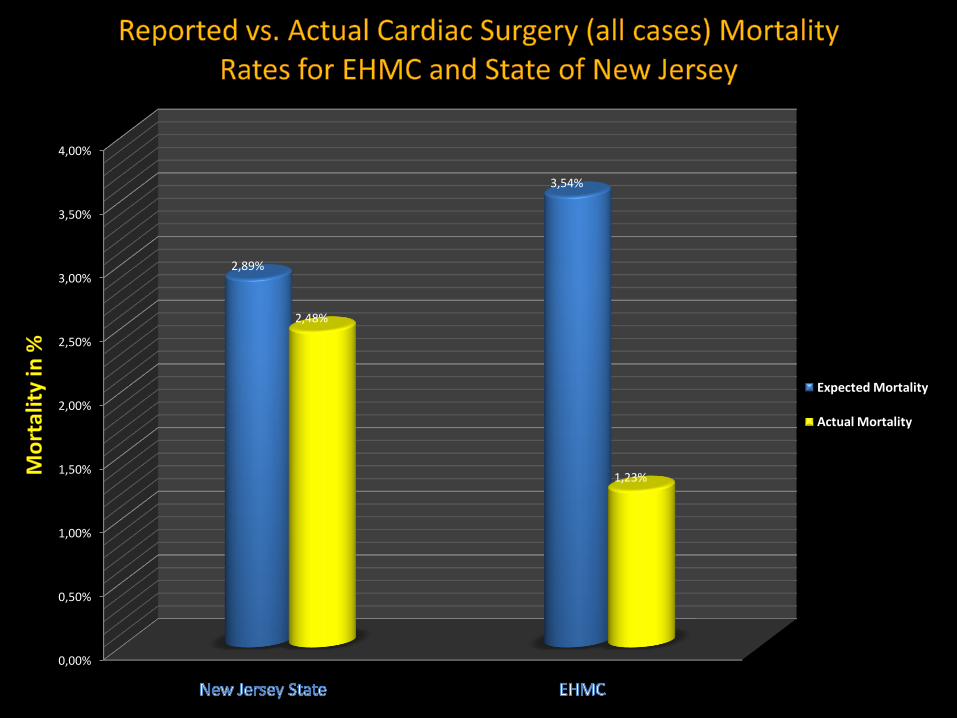
0,00%
0,50%
1,00%
1,50%
2,00%
2,50%
3,00%
3,50%
4,00%
2,89%
3,54%
2,48%
1,23%
Expected Mortality
Actual Mortality
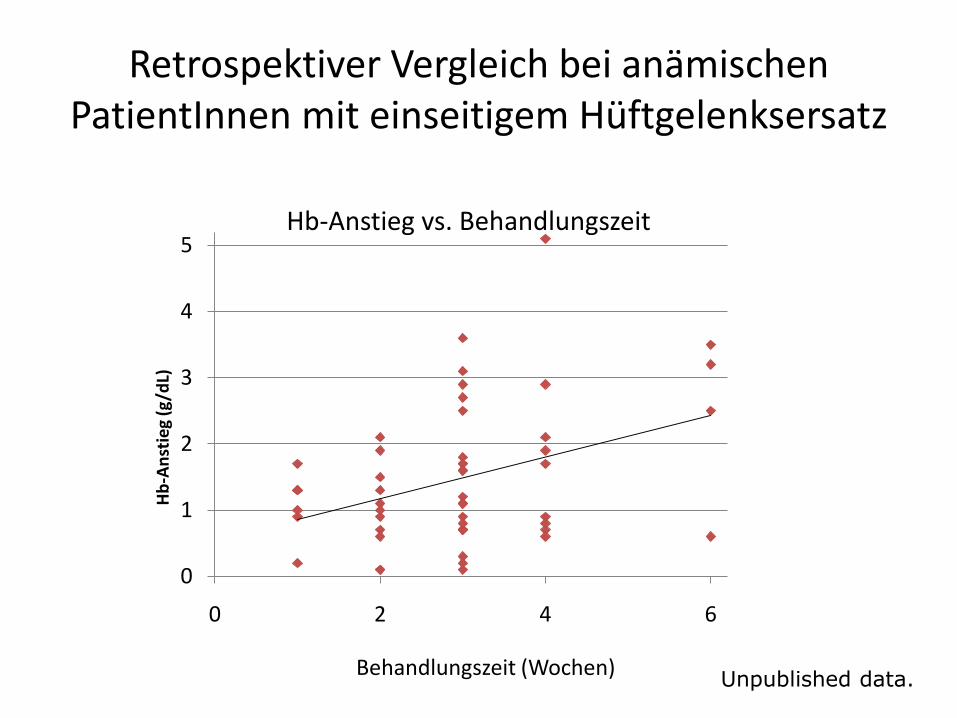
Retrospektiver Vergleich bei anämischen PatientInnen mit einseitigem Hüftgelenksersatz
%
Unpublished data.
n = 2x50 Patientinnen
0
1
2
3
4
5
0 2 4 6
Hb
-An
stie
g (g
/dL)
Behandlungszeit (Wochen)
Hb-Anstieg vs. Behandlungszeit
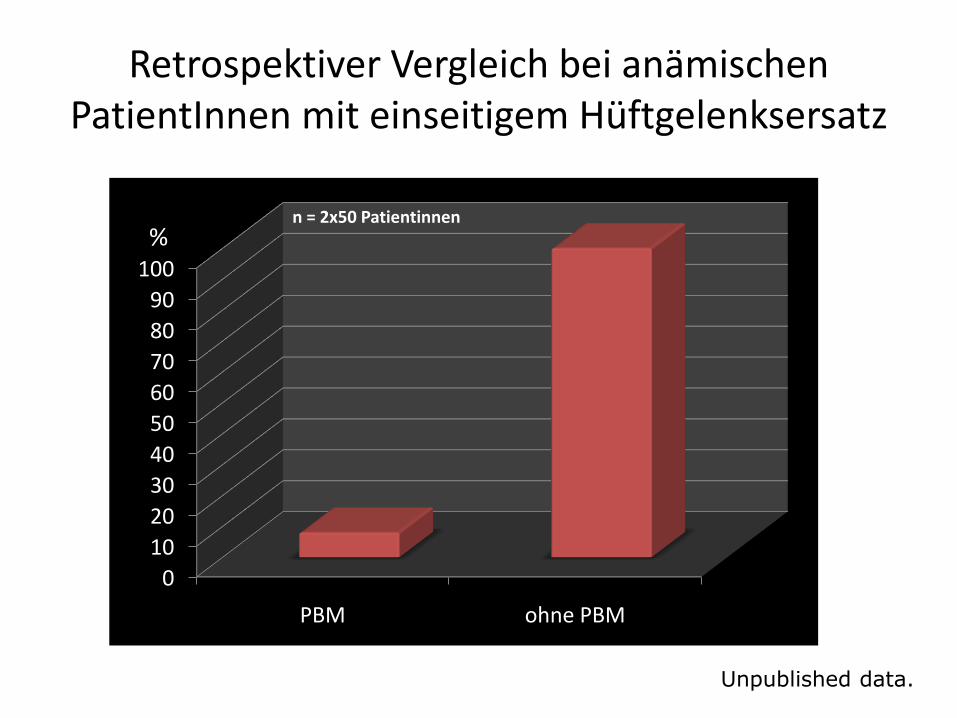
Retrospektiver Vergleich bei anämischen PatientInnen mit einseitigem Hüftgelenksersatz
0
10
20
30
40
50
60
70
80
90
100
PBM ohne PBM
%
Unpublished data.
n = 2x50 Patientinnen
Study evaluating PBM Outcomes
Compared a cohort of 586 pts undergoing
isolated CABG at an institution with a
developed PBM Program (PBMP) with a
propensity-score matched cohort of 586
pts from institutions without a PBMP
Isolated CABG includes elective & urgent and primary & redo procedures
© Axel Hofmann AIC Graz 09-2010
PBM strategies used:
1. Preop haemoglobin optimisation
2. Intraop ANH and Intra & Postop cell salvage
3. Meticulous surgical technique
4. Endovascular vein harvesting
5. Point-of-care coagulation testing
6. Targeted haemostatic therapy
7. Tolerance of perioperative anaemia (60 – 70 g/L depending on patient-specific physiology)
© Axel Hofmann AIC Graz 09-2010
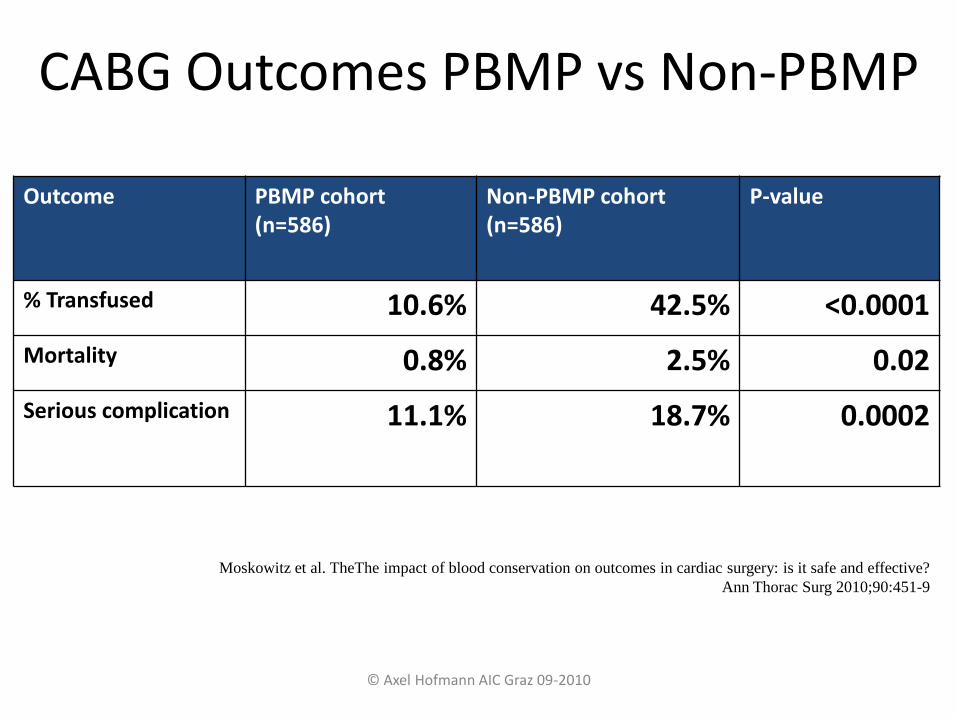
CABG Outcomes PBMP vs Non-PBMP
Outcome PBMP cohort (n=586)
Non-PBMP cohort (n=586)
P-value
% Transfused 10.6% 42.5% <0.0001
Mortality 0.8% 2.5% 0.02
Serious complication 11.1% 18.7% 0.0002
Moskowitz et al. TheThe impact of blood conservation on outcomes in cardiac surgery: is it safe and effective?
Ann Thorac Surg 2010;90:451-9
© Axel Hofmann AIC Graz 09-2010
Postgraduate Hochschulkurs Universität GRAZ
Dauer: 3 Semester einschließlich PBM-Project
Kosten: 20 Ek‘s pro Semester u. Teilnehmer
Leiter: Gombotz, Kurz, Lanzer
Beginn: Herbst 2011

69