squamous cell carcinoma antigen in patients with cutaneous disorders
TRANSCRIPT

Yolume22Number 4April 1990
eralisata (Ehrmann) mit cerebrovaculiirer Beteiligung(Herman-Sneddon). Aktuel Dermato1 1985;11:17-21.
20. Schriftenreihe des Bundesministers fUr Jugend, Familieund Gesundheit. Daten des Gesundheitswesens, Ausgabe1985.
21. Doring G. Empfringnisverhiitung. Stuttgart: Thieme, 1983,22. Stephens WP, Ferguson JT. Livedo reticularis and cere·
brovascular disease. Postgrad Med J 1982;58:70-3.23. Rumpl E, Neuhofer J, PaIIua A, et al. Cerebrovascular le
sions and livedo reticularis (Sneddon's syndrome): a progressive cerebrovascular disorder? J Neurol 1985;231:32430.
24. Lewis T, Pickering GW. Observations upon maladies inwhich the blood supply to digits ceases intermittently orpermanently, and upon bilateral gangrene of digits: observations relevant to the so called "Raynaud's disease." ClinSci 1934;1:327-66.
25. Allen EY, Brown GE. Raynaud's disease: a critical reviewof minimal requisites for diagnosis. Am J Med Sci 1932;183-7.
Livedo racemosa
26. Kaha1eh MB, Sherer GK, Le Roy Ee. Endothelial injuryin scleroderma. J Exp Med 1979;149:1326-35.
27. Shanahan WR, Korn JR. Cytotoxic activity of sera fromscleroderma and other connective tissue diseases: lack ofcellular and disease specificity. Arthritis Rheum 1982;25:1391-5.
28. Meyer 0, Haim T, Dryll A, et al. Vascular endothelial cellinjury in progressive systemicsclerosis and other connectivetissue diseases. CUn Exp Rheumato11983;1:29-34.
29. Cohen S, Johnson AR, Hurd E. Cytotoxicity of serafrom patients with scleroderma. Arthritis Rheum 1983;26:170-8.
30. Deicher HFG, Drenk F, Hoffmann G. Identmcation of anLTB 4-protein complex as evidence of endothelial cell cytotoxic activity (ECA) in progressive systemic sclerosis(PSS). Z RheumatoI1987;46:196-7.
31. Drenk F, Lubach D, Schwabe C, et aI. Endothelial cytotoxic activity (ECA) in sera of patients with livedo race·mosa generalisata (Ehrmann). Arch Dermatol Res1987;279:415-7.
Squamous cell carcinoma antigen in patients withcutaneous disordersBruce Campbell, MB,BS,a and Brian De'Ambrosis, MB,BSbBrisbane, Queensland, Australia
Serum levels of the tumor marker squamous cell carcinoma antigen (TA-4) were examinedin patients with nonneoplastic dermatologic diseases. The majority of patients with significant disease had elevated levels of this antigen. The percentage of involved skin surface areacorrelated with serum squamous cell carcinoma antigen levels. Psoriasis and atopic dermatitis have different effects on squamous cell carcinoma antigen levels. Kidney failure alsocauses elevated levels. Squamous cell carcinoma antigen is not a reliable tumor marker in patients with squamous cell carcinoma at any site when these patients also have a cutaneousdisorder that involves more than 2% of the skin surface area or when they have kidney failure. (J AM ACAD DERMATOL 1990;22:639-42.)
Squamous cell carcinoma (SeC) antigen, alsoknown as tumor-associated antigen, or TA-4, is a
protein with a molecular weight of approximately48,000 daltons. In 1977 Kato and Torigoe1 developed a radioimmunoassay for a protein antigen ex-
From the Departments of Pathology" and Dermatology,b PrincessAlexandra Hospital.
Accepted for publication June 22, 1989.
Reprint requests: Brian De'Ambrosis, MB,BS, Department of Dermatology, Princess Alexandra Hospital, Ipswich Rd. Wooloongabba4102, Brisbane, Queensland, Australia.
16/1/14954
tractedfromsecoftheuterine cervix. The assay hasbeen used primarily as a tumor marker in patientswith sec of the cervix.2-4 Other reports examined
the use of this marker in patients with sec of othersites, including the lung5 and the head and neck.5-7
One preliminary study8 investigated its use in patients with sec of the skin and in a small numberof patients with nonmalignant disorders of the skin.
This study concluded that sce antigen levels wereelevated in patients with large primary SCC of the
skin and in patients with metastatic disease. secantigen levels were stated to be within the normallimits in patients with smaller nonmetastatic sce,Bowen's disease, and other non-SeC dermatoses.8
639

640 Campbell and De'Ambrosis
SERUM see Ag LEVEL (ng/m1 )
Journal of theAmerican Academy of
Dermatology
0.5 1.0 2.4 5.0 10.0 50.0
HEALTHY CONTROLS • • I~ I'e N=56
PSORIASIS ••• \ I ··1 ...\ • •• I • • N=26
ATOPIC DER"ATITIS .. \ I n. • A •• •• • • N=23
OTHER DISORDERSN=15• • • • ..• r.· • • •
<2~ SKIN AFFECTED
OTHER DISORDERS
>2S SKIN AFFECTED " •••• • y .. • • • N=19
Fig. 1. Serum see antigen levels in healthy control subjects and in four groups ofpatientswith dermatologic disorders.
Because sec antigen has been demonstrated innormal squamous epithelium~9, 10 we tested the hypothesis that sec antigen levels would be elevatedin nonneoplastic disorders that affected a significant part of the surface area of the skin.
PATIENTS AND METHODS
All new patients admitted to the dermatology department had blood drawn for see antigen level assay aftertheir consent was obtained. The severity of their diseasewas assessed as mild, moderate, or severe, and thepercentage of involved body surface area was estimatedby the Lund and Browder charts. 11 sec antigen levelswere determined by radioimmunoassay (Abbott Laboratories, N. Chicago, Ill.). The interassay coefficient ofvariation was 12.1% at sec antigen level of 3.6 ngjmland 7.4% at 9.7 ng/ml. sec antigen levels were also determined ina group of56 healthy hospital staffmembers.Because one previous study reported that patients withkidney failure may have elevated see antigen leve!s,6four patients with elevated plasma creatinine levels wereexcluded from the study. A separate evaluation of seeantigen levels in a small group of patients with varyingdegrees ofkidney failure butwithout evidence ofskin disease Or malignancy was also made.
RESULTS
Fig. 1shows data broken down into four categories for the control group and for the patients. Of the
healthy control subjects, 95% had sec antigen levels ofless than 2.4 ng/ml; this level was taken as thecutoff point between normal and abnormal levels.The majority of the patients (70%) had elevatedsecantigen levels. Patients with disorders affectingmore than 2% of their skin surface area were evenmore likely to have elevated sec antigen levels. Thepatients with limited areas ofcutaneous involvementincluded individual cases of pemphigus vulgaris, endogenous dermatitis, lichen planus, cutaneous leukocytoclastic vasculitis, livedoid vasculitis, cellulitisof the leg, bacterial folliculitis, contact irritant dermatitis, and keratoacanthoma centifugum marginatum, and six patients with leg ulcers.
We found a significant correlation between secantigen levels and percentage of skin surface areainvolved. When all the patients' data are consideredtogether, Pearson's correlation coefficient (r) is 0.51(p < 2 X 10-6). When the two largest patientgroupsare considered separately, a difference is found. Forpatients with atopic dermatitis, the correlation between sec antigen levels (r) and the percentage ofskin involvement is 0.77 (p < 2 X 10-5). For patients with psoriasis r = 0.44 (p < 0.03). Thus, although the degree of correlation between sec antigen levels and percentage skin involvement in boththese diseases is significant, the correlation is muchstronger in patients with atopic dermatitis. This can
Volume 22Number 4April 1990 sec antigen in skin disorders 641
2 I.- .,.-•
* SCG Ag,,35.3 ng/ml
tPSORIASIS
•40
•SCC Ag• •(ng/ml) ••
20 •.. •• •,.. •..-. ..50 100
SKIN %
10
8SCCAg(ng/mJ)6
4
•••
••
•••
50 100
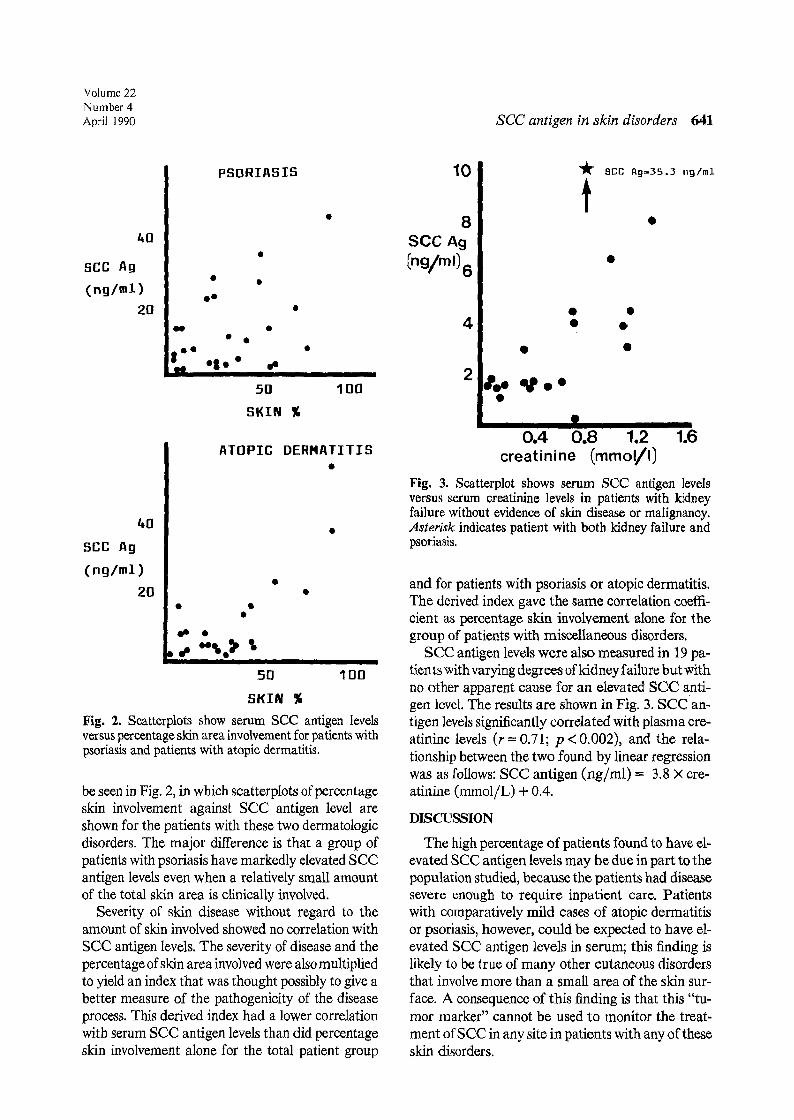
SKIN %Fig. 2. Scatterplots show serum see antigen levelsversus percentage skin area involvement for patients withpsoriasis and patients with atopic dermatitis.
be seen in Fig. 2, in which scatterplots of percentageskin involvement against sec antigen level areshown for the patients with these two dermatologicdisorders. The major difference is that a group ofpatients with psoriasis have markedly elevated secantigen levels even when a relatively small amountof the total skin area is clinically involved.
Severity of skin disease without regard to theamount of skin involved showed no correlation withsec antigen levels. The severity of disease and thepercentage ofskin area involved were also multipliedto yield an index that was thought possibly to give abetter measure of the pathogenicity of the diseaseprocess. This derived index had a lower correlationwith serum see antigen levels than did percentageskin involvement alone for the total patient group
40
SCC Ag
(ng/ml)
20
ATOPIC DERMATITIS
--
- -. •
0.4 0.8 1.2 1.6creatinine (mmoVI)
Fig. 3. Scatterplot shows serum sec antigen levelsverSus serum creatinine levels in patients with kidneyfailure without evidence of skin disease or malignancy.Asterisk indicates patient with both kidney failure andpsoriasis.
and far patients with psoriasis or atopic dermatitis.The derived index gave the same correlation coeffiw
cient as percentage skin involvement alone for thegroup of patients with miscellaneous disorders.
sec antigen levels were also measured in 19 patients with varying degrees ofkidney failure butwithno other apparent cause for an elevated see antigen level. The results are shown in Fig. 3. sec antigen levels significantly correlated with plasma creatinine levels (r =0.71; p <0.002), and the relationship between the two found by linear regressionwas as follows: sec antigen (ng/m!) = 3.8 X creatinine (mmol/L) + 0.4.
DISCUSSION
The high percentage of patients found to have elevated sec antigen levels may be due in part to thepopulation studied, because the patients had diseasesevere enough to require inpatient care. Patientswith comparatively mild cases of atopic dermatitisor psoriasis, however, could be expected to have elevated see antigen levels in serum; this finding islikely ta be true of many other cutaneous disordersthat involve more than a small area of the skin surface. A consequence of this finding is that this "tumor marker" cannot be used to monitor the treatment ofsee in any site in patients with any oftheseskin disorders.

642 Campbell and De'Ambrosis
Disorders that affected less than 2% of the skinarea generally had minimal effect on theserum secantigen levels, except for a rare variant of keratoacanthoma in a patient who had a level of 6.1 ng/ml. This finding is in accord with the significant degree of correlation found between see antigen levels and percentage of skin surface area involved bythe disease process. This general phenomenon isfound when all the diseases are grouped together.
Immunofluorescence studies have demonstratedsee antigen to be present mainly in the intermediate layers of the squamous epithelium of the uterinecervix,9, 10 although the intracellular localization ofsee antigen is not well defined. Immunofluorescence studies have suggested that the antigen is inthe cytoplasm rather than on the cell surface,lo andthus increased plasmalevels are most likely to be dueto cell death and lysis or to increase in the permeability of the cell membrane that allow escape of theantigen into the circulation. Alternatively, cutaneous diseases may lead to an increased production ofsee antigen by epithelial cells, similar to theincreased production of acute phase reactant proteins by hepatocytes under the influence of certaincytokines. 12
The lesser degree of correlation between seeantigen levels and skin involvement in psoriasiscompared with atopic dermatitis may be due to differences in the pathogenesis of these diseases. Psoriasis is a disease that is known to increase the cellturnover rate in apparently clinicallyuninvolved skinas well as in the clinical lesions. 13 Variations in overall. epidermal cell kinetics may explain the poorercorrelation with serum see antigen levels in thisdisease. The lack of correlation between disease severity and see antigen levels was not expected andmay be due to the subjective clinical assessment ofdisease severity as a variable that is independent ofthe area of skin involved.
The highest serum levels of sec antigen wereseen in generalized atopic dermatitis with an acuteexacerbation due to bacterial infection, unstableacute inflammatory psoriasis, and in erythrodermicatopic dermatitis. A common finding in the aboveconditions is marked erythema. The associatedincreased cutaneous blood supplycould allow greaterabsorption of see antigen from the epidermis intothe systemic circulation. A similar mechanism maybe important in explaining the high serum sec antigen levels in psoriasis.
Journal of theAmerican Academy of
Dermatology
The findings of elevated sec antigen levels inpatients with kidney failure confirms that of Molinaet al.6 and contradicts assertions made by others.s
The simultaneous presence of skin disease (psoriasis) and kidney failure had a synergistic effect on elevating sec antigen levels as shown by the patientdenoted by an asterisk in Fig. 3.
This study has demonstrated that serum seeantigen levels are elevated in many patients with cutaneous disorders, particularly those diseases withan inflammatory component that affect more than2% ofthe body surface area. sec antigen cannot beused as a tumor marker in patients with these typesof dermatologic disease.
We acknowledge the helpful discussions we had withDr. Graeme L. Beardmore during the preparation of thismanscript. The sec antigen kits used in this study weredonated by Abbott Laboratories, North Chicago, Illinois.REFERENCES
1. Kato H, Torigoe T. Radioimmunoassay for tumor antigenof human cervical squamous cell carcinoma. Cancer1977;40:1621-8.
2. Kato H, Miyauchi F, Morioka H, et a1. Tumor antigen ofhuman cervical carcinoma: correlation of circulating levelswith disease progress. Cancer 1979;43:585-90.
3. Kato H, Morioka H, Aramaki S, et a1. Prognostic significance of the tumor antigen TA-4 in squamous cell carcinoma of the uterine cervix. Am J Obstet Gynecol1983;145:350-4.
4. Maruo T, Shibata K, Kimura A, et a1. Tumor-associatedantigen, TA-4, in the monitoring of the effects of therapyfor squamous cell carcinoma of the uterine cervix. Cancer1985;56:302-8.
5. Mino N, lio A, Hamamoto K. Availability of tumorantigen 4as a marker of squamous cell carcinoma of thelung and other organs. Cancer 1988;62:730-4.
6. Molino R, Torres X, Filella PJ, et a1. Serum SCC antigenin patients with head and neck tumors. J Tumor MarkerOncol 1987;2:277-82.
7. Yoshimura Y, Harada T, aka M, et a!. Squamous cellcarcinoma antigen in the serum of oromaxillary cancer. IntJ Oral Maxillofac Surg 1988;17:49-53.
8. Yagi H, Danno K, Maraguchi Y, et a!. Significance ofsquamous cell carcinoma (SCC)-related antigens in cutaneous SCc. Arch Dermatol1987;123:902-6.
9. Ueda G, Inoue Y, Yamasaki M, et a1. Immunohistochemical demonstration of tumor antigen TA-4 in gynecologictumors. lnt J Gynecol PathoI1984;3:291-8.
10. Suehiro Y, Kato H, Michihiro N, et a1. Flow cytometricanalysis of tumor antigen TA-4 in cervical cytologic specimens. Cancer 1986;57:1380-4.
11. Lund ce,Browder NC. The estimation of areas of burns.Surg Gynecol Obstet 1944;79:352-8.
12. Nelson DS, Geczy CL. Lymphokines, monokines and othercytokines. Aust N Z J Med 1985;15:285-90.
13. Gelfant S, Ozawa A, Chalker DK, et a1. Circadian rhythmsand differences in epidermal and dermal cell proliferationin uninvolved and involved psoriatic skin in vivo. J InvestDermatol 1982;78:58-62.