„wer heute nicht handelt, kann - adka.de · mythos auf wunsch der operateure wird gelegentlich...
TRANSCRIPT
Apotheke
Zentrum für Anästhesie und Intensivmedizin
„Wer heute nicht handelt, kann
morgen nicht mehr heilen“ Motto des Weltgesundheitstages 2011
Perioperative Antibitotika-Prophylaxe
Heike Hilgarth
Fachapothekerin für Klinische Pharmazie
Diploma in Pharmacy Practice
ABS ExperteUniversitätsklinikum Hamburg-Eppendorf

ADKA Mannheim 28.-30.05.2015 Heike Hilgarth ([email protected]) 2
Rate der SSI pro Operationsgebiet
aus Präsentation Bratzler, Strategies for the Prevention of Surgical Site Infections Review of New Multi-
specialty Society Guideline 15. August 2012
Frage 1
ADKA Mannheim 28.-30.05.2015 Heike Hilgarth ([email protected]) 3
Die Wirkung der perioperativen Antibiotikaprophylaxe (PAP) ist abhängig
vom Zeitpunkt der Gabe und der Halbwertszeit des Antibiotikums. Wann
und wie lange sollte die PAP gegeben werden?
a) Bei ungestörter gastrointestinaler Resorption ist eine PAP am
Vorabend ausreichend effektiv.
b) Bei einem Blutverlust von > 1l ist die erneute intraoperative Gabe der
PAP sinnvoll.
c) Wird Cefuroxim angewendet, wird intraoperativ nach 90 min eine
wiederholte Dosierung empfohlen.
d) Die PAP ist bis zu 30 min nach Operationsbeginn vergleichbar effektiv,
wie 30 min vor Beginn der Operation.
B: Eine Applikation nach Wundverschluss hat keinen Einfluss auf die Infektions
-rate. Bei starkem Blutverlust (>1 L) oder länger dauernden Operationen muss
in Abhängigkeit von der Halbwertzeit des applizierten Antibiotikums eine
Folgedosis verabreicht werden. (Leitlinie 029-022 – Perioperative
Antibiotikaprophylaxe) (nach P
unke
et
al A
nae
sth
esis
t2014 ·
63:7
3–
86
)
Frage 3
ADKA Mannheim 28.-30.05.2015 Heike Hilgarth ([email protected]) 4
Unter welchen Bedingungen sollte die PAP wiederholt werden?
a) Wenn die OP-Dauer die doppelte Halbwertzeit des Antibiotikums
überschreitet
b) Nach einer OP-Dauer von mehr als 4 Stunden
c) Postoperativ, wenn eine Nachbeatmung notwendig wird
e) Bei Konversion von Laparoskopie zu Laparotomie
A: Eine einmalige Gabe ist bei in der Regel bei Operationen von unter zwei
Stunden ausreichend, bei länger andauernden Eingriffen sollte eine Wiederholung
in Abhängigkeit von der Halbwertszeit erfolgen. Bei laparoskopischen Eingriffen
kann bei fehlendem Infektionsrisiko auf eine PAP verzichtet werden. Deshalb
keine Wiederholung sondern Erstgabe! Bei einem Verfahrenswechsel steigt bei
z.B. einer Cholecystektomie das postoperative Infektionsrisiko um den Faktor 3,5
bis 4,7 (Wacha 2010)
(nach Punke et al Anaesthesist 2014 · 63:73–86)

ADKA Mannheim 28.-30.05.2015 Heike Hilgarth ([email protected]) 5

Redosing

Mythos
Auf Wunsch der Operateure wird gelegentlich die
Antibiotikaprophylaxe auf 3, 5 oder 7 Tage post-operativ
ausgedehnt. In den vielen vergleichenden Studien korrelierte eine
über die Zeitdauer der Operation verlängerte Prophylaxe
jedoch nicht mit einer geringeren Infektionsrate, sondern erhöhte
vielmehr die Rate von Neben-wirkungen, Resistenzentwicklung und
der Entstehung einer Infektion mit Clostridium difficile.
ADKA Mannheim 28.-30.05.2015 Heike Hilgarth ([email protected]) 7
Au
sL
em
me
n2
013A
nästh
esio
lInte
nsiv
me
dN
otf
allm
edS
chm
erz
the
r2
01
3;4
8:5
18–
523


Frage 2
ADKA Mannheim 28.-30.05.2015 Heike Hilgarth ([email protected]) 9
Wann besteht die Indikation, eine PAP im Sinne einer Therapie
weiterzuführen?
a) kontaminierte, nicht infizierte Wunde nach einem Verkehrsunfall
b) Appendicitis acuta mit lokaler Peritonitis
c) Operation am Neurokranium
d) Implantationen einer Endoprothese am Hüftgelenk
B: Bei bestehender Infektion bzw. bei fehlender vollständiger Beseitigung
des Infektionsherdes sollte eine Therapie eingeleitet werden.
(nach P
unke
et
al A
nae
sth
esis
t2014 ·
63:7
3–
86
)

„Diese prolongierten Therapien sind teuer, unnütz und
gefährlich“, warnte Dr. Christian Eckmann, Chefarzt
der Klinik für Allgemein-Viszeral- und Thoraxchirurgie
am Klinikum Peine. „Ein Bakterium hat eine
Vermehrungszeit von 20 Minuten. Innerhalb von 3
Tagen geben Sie dem Bakterium 200 Generationen
Zeit, einen Resistenzmechanismus zu entwickeln.
PD
Dr.
Ch
ristia
n E
ckm
an
n, K
linik
um
Pe
ine
ADKA Mannheim 28.-30.05.2015 Heike Hilgarth ([email protected]) 10

Top 10 Antiinfektiva– stationär
Germap 2012
ADKA Mannheim 28.-30.05.2015 Heike Hilgarth ([email protected]) 12

ADKA Mannheim 28.-30.05.2015 Heike Hilgarth ([email protected]) 13

Frage 4
ADKA Mannheim 28.-30.05.2015 Heike Hilgarth ([email protected]) 14
Bei primär aseptischen Operationen, die nach der allgemeinen Wund-
klassifikation als sauber bezeichnet werden,
a) ist eine PAP nicht indiziert.
b) Ist die Notwendigkeit einer PAP für spezielle Patientengruppen
/Risikofatoren zu prüfen
c) ist eine PAP bei hoher Resistenzentwicklung im Krankenhaus
empfehlenswert.
d) wird bei der Implantation von Fremdmaterial eine PAP empfohlen.
B und D: bei sauberen Eingriffen mit Infektionsgefährdung auf Grund patienteneigener
Risiken und als Folge erheblicher Morbidität oder Letalität, z. B. Eingriffe bei
immunsupprimierten Patienten, bei Patienten mit schweren Grunderkrankungen, bei
Patienten mit hohem ASA-Score, Vorbestrahlung, Unterkühlung.(AWMF Leitlinie Perioperative
Prophylaxe)
(nach Punke et al Anaesthesist 2014 · 63:73–86)

Kosten für nicht leitlinien-gerechte PAP zwischen 12.000 US$- 26.000 US$
Berechnete Einsparungen bei Leitlinien-entsprechendem Einsatz bis US
$6.1 Mio (Belgien 1998)
Compliance(gesamt) der Operateure mit den Empfehlungen 0 – 72%
Hauptgründe: ungeeignete Auswahl, zeitgerechte Gabe, Dauer der
Prophylaxe
Bessere Adhärenz hinsichtlich Indikation und Dosierung
ADKA Mannheim 28.-30.05.2015 Heike Hilgarth ([email protected]) 15

Indikation: 68- 100% Adhärenz
Auswahl: < 70% Adhärenz
Zeitpunkt der Gabe: 22- 100 % Adhärenz
Dauer: 0-98% Adhärenz; Mehrheit < 50%
Dosis: >80% Adhärenz
ADKA Mannheim 28.-30.05.2015 Heike Hilgarth ([email protected]) 16
GRÜNDE!
Neueste lokale POP-Version nicht in aktueller Form vorliegend; Verschiedene
Meinungen innerhalb der Operateure; Logische Abläufe – Station – OP; Vergessen, dass
es Empfehlungen gibt; Unterschätzung des Infektionsrisikos
ADKA Mannheim 28.-30.05.2015 Heike Hilgarth ([email protected]) 17

Fragen 5 und 6
ADKA Mannheim 28.-30.05.2015 Heike Hilgarth ([email protected]) 18
Welches Antibiotikum kommt einzeln oder in Kombination in der
Regel nicht zur PAP während chirurgischen Eingriffen am Kolon
infrage?
a) Cefuroxim
b) Metronidazol
c) Ampicillin/BLI
d) Gentamycin
e) Vancomycin
Ein 73jähriger Patient soll in Narkose gastroskopiert werden. Welche
Entscheidung treffen Sie bezüglich der PAP?
a) Cephalosporin der 2. Generation + BLI
b) Cephalosporin der 2. Generation + Vancomycin
c) Eine PAP ist nicht notwendig
d) Aminopenicillin plus Gentamycin
(nach P
unke
et
al A
nae
sth
esis
t2014 ·
63:7
3–
86
)

Frage 7
ADKA Mannheim 28.-30.05.2015 Heike Hilgarth ([email protected]) 19
Eine 32-jährige vormals gesunde Patientin erkrankt an einem
Mammakarzinom und soll operiert werden. Welche Überlegungen
treffen Sie bezüglich der PAP?
a) Nach der Klassifikation von Cruse handelt es sich nicht um einen
sauberen Eingriff.
b) Eine PAP ist aufgrund der Tumorerkrankung indiziert.
c) Da die Patientin keine Nebenerkrankungen hat, kann auf ein PAP
verzichtet werden.
d) Die Indikation einer PAP ergibt sich nur bei simultaner axillärer
Lymphadenektomie.
B: Alle Patienten mit einer Karzinom bedingten Intervention besitzen ein
signifikant erhöhtes post-operative Infektionsrisiko.
(nach P
unke
et
al A
nae
sth
esis
t2014 ·
63:7
3–
86
)

Frage 8
ADKA Mannheim 28.-30.05.2015 Heike Hilgarth ([email protected]) 20
Wie ist mit der PAP umzugehen, wenn der Patient bereits eine antimikrobielle
Therapie erhält?
a) OP-spezifische Eskalation der Therapie bei nicht ausreichender Abdeckung
des Eingriffes
b) An die Operation angepasste PAP und Aussetzen der bisherigen
antimikrobiellen Therapie
c) Ergänzung der präoperativen antimikrobiellen Therapie durch Gabe der
PAP für 5-7 Tage
d) Wechsel auf ein Carbapenem bei endoprothetischen Operationen
e) Pseudomonas wirksame PAP unabhängig von Operation und
Wundklassifikation
A: Patients receiving therapeutic antimicrobials for a remote infection before surgery should
also be given antimicrobial prophylaxis before surgery to ensure adequate serum and tissue
levels of antimicrobials with activity against likely pathogens for the duration of the operation. If
the agents used therapeutically are appropriate for surgical prophylaxis, administering an extra
dose within 60 minutes before surgical incision is sufficient. Otherwise, the antimicrobial
prophylaxis recommended for the planned procedure should be used. For patients with
indwelling tubes or drains, consideration may be given to using prophylactic agents active
against pathogens found in these devices before the procedure, even though therapeutic
treatment for pathogens in drains is not indicatedat other times. (Bratzler 2013)
(na
ch
Pu
nke
et
al A
na
esth
esis
t2
01
4 ·
63
:73
–86
)

Frage 9
ADKA Mannheim 28.-30.05.2015 Heike Hilgarth ([email protected]) 21
Eine 68jährige Patientin soll wegen einer akuten Cholecystitis operiert
werden. Sie war bereits im Vormonat hospitalisiert und musste damals wegen
einer Pseudomonas aeruginosa Pneumonie für drei Tage maschinell beatmet
werden. Welche PAP wählen Sie?
a) Cephalosporin der Gruppe 3a + Metronidazol
b) Acylaminopenicillin + BLI
c) Aminopenicilline
d) Moxifloxacin
e) Levofloxacin + Teicoplanin
B: Risikopatientin:
1) mit stattgehabter Abx Therapie, 2) KH-Aufenthalt, 3) Notfall-OP 4) ggfs.
Gallensteine (bis zu 90% der Cholecystitiden) 5) Fieber
Gallenwegschirurgie bei vorliegenden Risikofaktoren: Acylaminopenicillin/BLI
(Evidenzgrad Ia, Empfehlungsgrad A) Cephalosporin3A+Mteronidazol (Evidenzgrad
Ia, Empfehlungsgrad B) fehlender Pseudomonas-Abdeckung (PEG 2010)
(nach Punke et al Anaesthesist 2014 · 63:73–86)



Eine Idee...
HNO 2015 · 63:118–124 DOI 10.1007/s00106-014-2946-x
ADKA Mannheim 28.-30.05.2015 Heike Hilgarth ([email protected]) 24

Initiative der Chirurgen
ADKA Mannheim 28.-30.05.2015 Heike Hilgarth ([email protected]) 25
http://www.dgav.de/arbeitsgruppen/allgemein-und-viszeralchirurgische-infektionen/initiative-zum-
antibiotikaverbrauch.html (4.06.2015)

htt
p:/
/ww
w.d
ga
v.d
e/a
rbe
itsg
rup
pe
n/a
llge
me
in-u
nd
-vis
ze
ralc
hir
urg
isch
e-i
nfe
ktio
nen
/in
itia
tive
-zu
m-a
ntib
iotika
ve
rbra
uch
.htm
l
ADKA Mannheim 28.-30.05.2015 Heike Hilgarth ([email protected]) 26
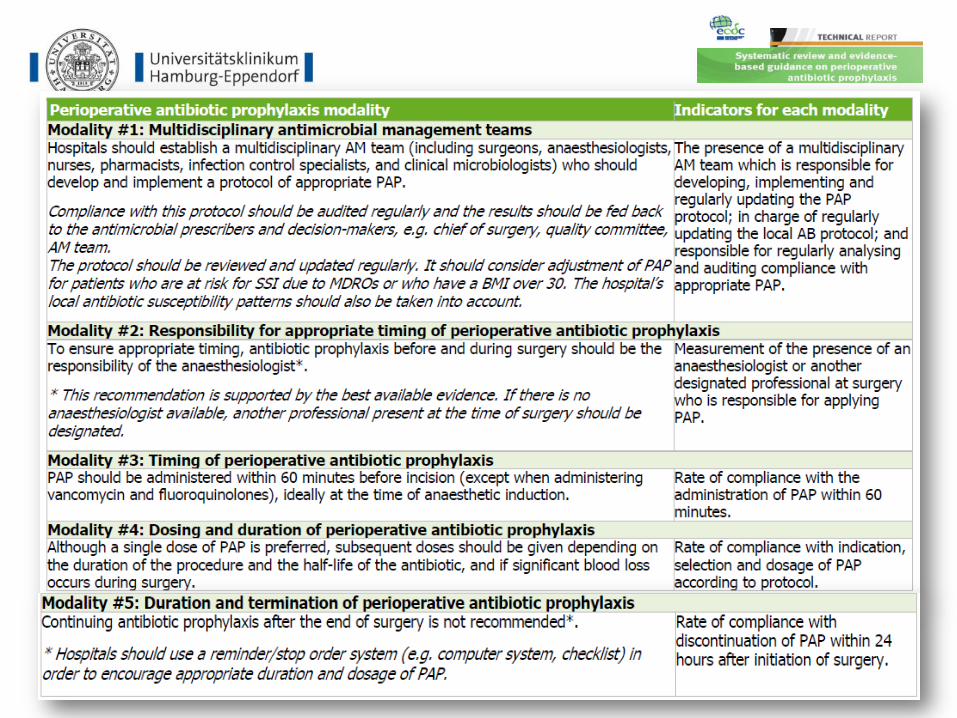
Initiative der Chirurgen
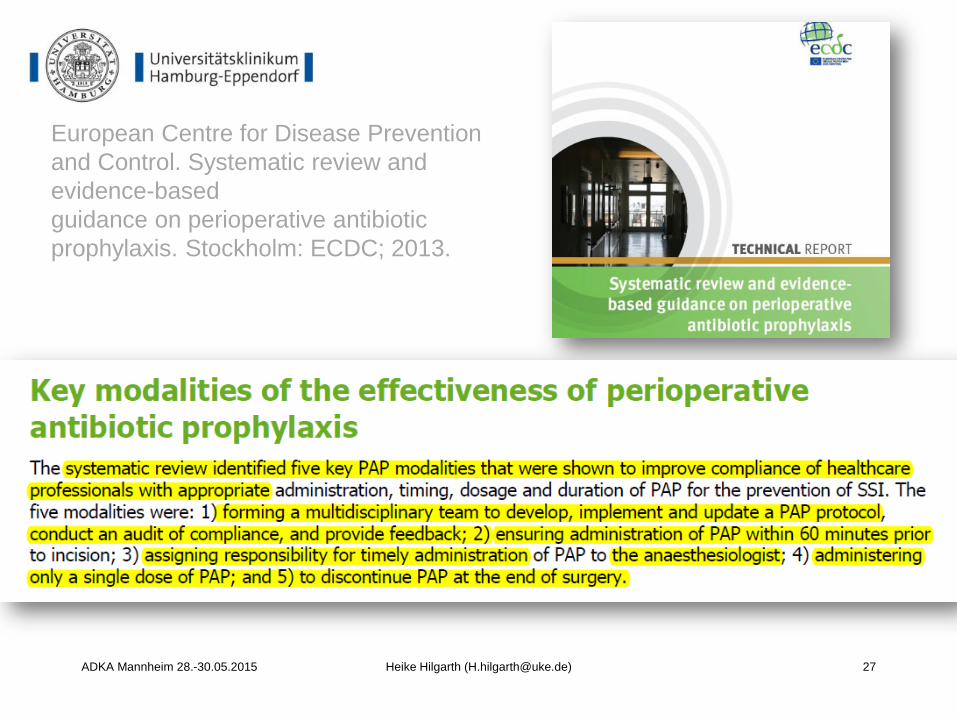
European Centre for Disease Prevention
and Control. Systematic review and
evidence-based
guidance on perioperative antibiotic
prophylaxis. Stockholm: ECDC; 2013.
ADKA Mannheim 28.-30.05.2015 Heike Hilgarth ([email protected]) 27
ADKA Mannheim 28.-30.05.2015 Heike Hilgarth ([email protected]) 28

ADKA Mannheim 28.-30.05.2015 Heike Hilgarth ([email protected]) 29

Pearls for Practice I
Clostridium difficile
Surgical prophylaxis can also predispose patients to
Clostridium difficile-associated colitis.(81) Risk factors for
development of C. difficile-associated colitis include
longer duration of prophylaxis or therapy and use of
multiple antimicrobial agents.(85) Limiting the duration of
antimicrobial prophylaxis to a single preoperative dose
can reduce the risk of C. difficile disease.
ADKA Mannheim 28.-30.05.2015 Heike Hilgarth ([email protected]) 30
Am
J H
ea
lth
-SystP
ha
rm. 2
01
3; 7
0:1
95
-28
3

The question of what antimicrobial surgical prophylaxis to
use for patients known to be colonized or recently
infected with multidrugresistant pathogens cannot be
answered easily or in a manner that can be applied
uniformly to all patient scenarios. Whether prophylaxis
should be expanded to provide coverage for these
pathogens depends on many factors, including the
pathogen, its antimicrobial susceptibility profile, the host,
the procedure to be performed, and the proximity of the
likely reservoir of the pathogen to the incision and
operative sites.
Am
J H
ea
lth
-SystP
ha
rm. 2
01
3; 7
0:1
95-2
83
ADKA Mannheim 28.-30.05.2015 Heike Hilgarth ([email protected]) 31
Pearls for Practice II
MDRE

Ta
ylo
r, A
. K
. e
t a
l. T
he J
ourn
al o
f U
rolo
gy 1
87
, 1
27
5–1279
(201
2).
ADKA Mannheim 28.-30.05.2015 Heike Hilgarth ([email protected]) 32

ADKA Mannheim 28.-30.05.2015 Heike Hilgarth ([email protected]) 33

Allergy to b-lactam antimicrobials may be a consideration
in the selection of surgical prophylaxis. The b-lactam
antimicrobials, including cephalosporins, are the
mainstay of surgical antimicrobial prophylaxis and are
also the most commonly implicated drugs when allergic
reactions occur. Confusion about the definition of true
allergy among patients and practitioners leads to
recommendations for alternative antimicrobial therapy
with the potential for a lack of efficacy, increased costs,
and adverse events.
Am
J H
ea
lth
-SystP
ha
rm. 2
01
3; 7
0:1
95
-28
3
ADKA Mannheim 28.-30.05.2015 Heike Hilgarth ([email protected]) 34
Pearls for Practice III
Allergie

http
://ww
w.a
shp
.org
/su
rgic
al-g
uid
elin
es
ADKA Mannheim 28.-30.05.2015 Heike Hilgarth ([email protected]) 35
Am
J H
ea
lth
-SystP
harm
—V
ol 7
0 F
eb
1, 2
01
3

However, in obese patients, especially those who are morbidly
obese, serum and tissue concentrations of some drugs may differ
from those in normal-weight patients because of pharmacokinetic
alterations that depend on the lipophilicity of the drug and other
factors.(101) Limited data are available on the optimal approach to
dosing of antimicrobial agents for obese patients. (102,103) If
weight-based dosing is warranted for obese patients, it has not been
determined whether the patient’s ideal body weight or total
(i.e.,actual) body weight should be used. In theory, using the ideal
body weight as the basis for dosing a lipophilic drug (e.g.,
vancomycin) could result in subtherapeutic concentrations in serum
and tissue, and the use of actual body weight for dosing a
hydrophilic drug (e.g., an aminoglycoside) could result in excessive
concentrations in serum and tissue.
Am
J H
ea
lth
-SystP
ha
rm. 2
01
3; 7
0:1
95-2
83
ADKA Mannheim 28.-30.05.2015 Heike Hilgarth ([email protected]) 37
Pearls for Practice IV
Übergewicht

Übergewicht
1989 (Forse et al Surgery. 1989;106:750-6)
- Cefazolin 2g was used instead of 1g, with a decrease of SSI from 16.5% to
5.6%
- noted a 16.5% SSI- incidence in patients with MO undergoing clean-
contaminated surgery, compared with 2.5% in a non-obese group
2012: (Ho et al SURGICAL INFECTIONS Volume 13, Number 1, 2012)
- SSI-Rate zwischen 1,3 und 22% berichtet
- A single 2-g dose of cefazolin appears to provide antibiotic exposures sufficient
for most common general surgical procedures of < 5-h duration, regardless of
BMI
- protective duration of fT>MIC of 70%, the time to redosing would be 5h
ADKA Mannheim 28.-30.05.2015 Heike Hilgarth ([email protected]) 38

ADKA Mannheim 28.-30.05.2015 Heike Hilgarth ([email protected]) 39
Exp
ert
Re
v P
harm
acoe
con
om
ics O
utc
om
es R
es. 2
01
0;1
0(3
):3
17
-328.

Zusammenfassung
Lokale Leitlinien erstellen im TEAM anhand der
vorhandenen Empfehlungen
Leitlinien überprüfen und Feedback geben
Leitlinien kommunizieren (Schulung, QM etc.)
Optimale Bedingungen schaffen (Verfügbarkeit der
Empfehlung und der Medikamente; Review auf Station)
ADKA Mannheim 28.-30.05.2015 Heike Hilgarth ([email protected]) 40

ADKA Mannheim 28.-30.05.2015 Heike Hilgarth ([email protected]) 41
Vielen Dank!
Für Fragen und Literatur [email protected]