patho ilben
TRANSCRIPT

8/3/2019 patho ilben
http://slidepdf.com/reader/full/patho-ilben 1/5
PATHOPHYSIOLOGY
Non-modifiable
Age – 77 years old
Gender – Male
Previous attack of MI (April 2011)
Race: Asian 1 of 100
Heredity: Hypertension
Modifiable
Anemia
Diabetes mellitus
Alcoholism
Smoking (1 pack X10)
Low activity
Activation of latelet
Formation of thrombus
Narrows or blockage of
cardiac artery
Emboli formation
Ischemia of tissue inThe region supplied by
coronary artery
ECG: 5/24/11Cannot r/oinferolateral wall
ischemia
Angina
Predisposing factors to contribute to
blood vessel wall injury and change in
condition of Coronary Artery by plaque
formation
Embolus travels to the heart
Embolus travels to the heart
Decreased oxygen supply tocardiac muscle resulting
anaerobic mechanism
Myocardial Injury leading tocell death
MYOCARDIALCARDIACMARKERS:↑ Troponin I:
Embolus travels to the brain
Blood flow obstructed bythrombus formation
Decrease Cerebral Perfusion
Cerebral Tissue Necrosis
CVD INFARCT
SIGNS AND SYMPTOMS
Impaired motor functions: unilaterallimb weaknessLeft sided hemiparesisDecreased Level of ConsciousnessHeadacheVision Disturbance: Ptosis
Esomolol 10mg IV now
Citicoline 1 IV 8
O2 @ 10LPM via facemask
8/3/2019 patho ilben
http://slidepdf.com/reader/full/patho-ilben 2/5
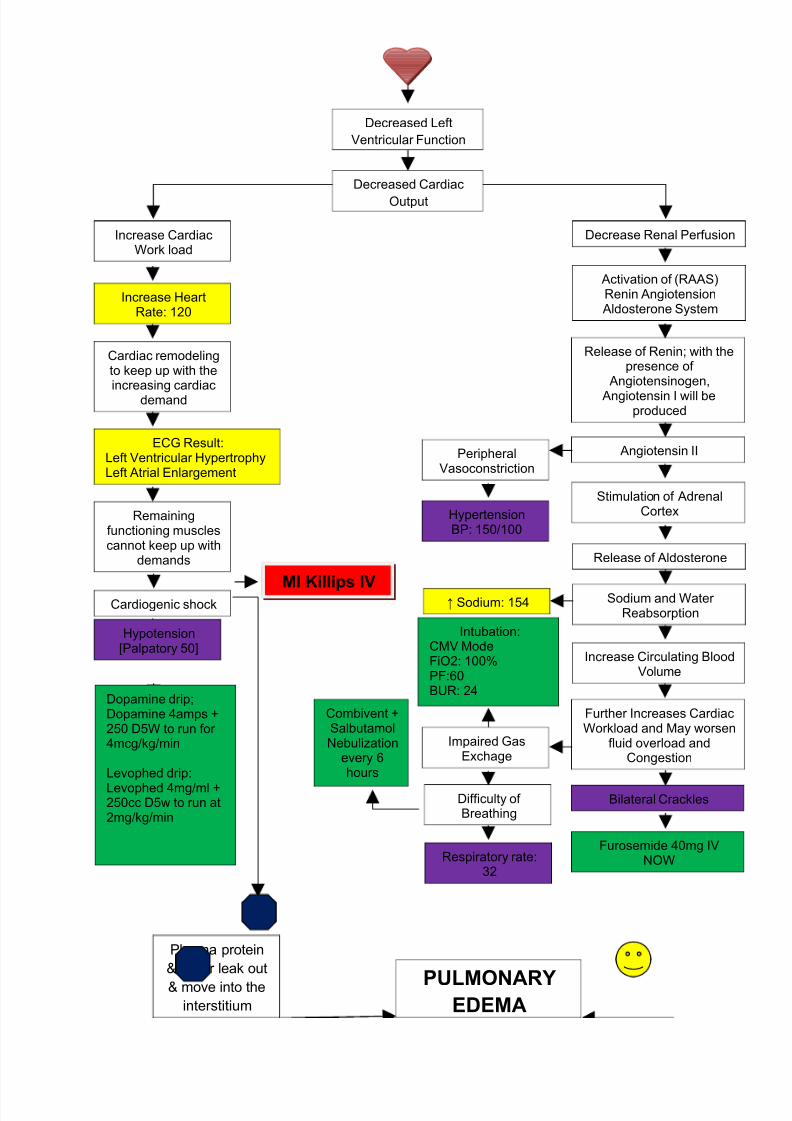
Plasma protein
& water leak out
& move into the
interstitiumPULMONARY
EDEMA
Decreased Left
Ventricular Function
Decreased Cardiac
Output
Decrease Renal Perfusion
Activation of (RAAS)Renin AngiotensionAldosterone System
Release of Renin; with thepresence of
Angiotensinogen,
Angiotensin I will beproduced
Angiotensin II
HypertensionBP: 150/100
Stimulation of AdrenalCortex
Release of Aldosterone
Sodium and Water Reabsorption
Increase Circulating BloodVolume
Further Increases CardiacWorkload and May worsen
fluid overload andCongestion
Bilateral Crackles
PeripheralVasoconstriction
↑ Sodium: 154
Increase CardiacWork load
Increase HeartRate: 120
Cardiac remodelingto keep up with theincreasing cardiac
demand
ECG Result:Left Ventricular HypertrophyLeft Atrial Enlargement
Furosemide 40mg IVNOW
Remainingfunctioning musclescannot keep up with
demands
Impaired GasExchage
Respiratory rate:32
Difficulty of Breathing
Intubation:CMV ModeFiO2: 100%PF:60BUR: 24
Combivent +SalbutamolNebulization
every 6hours
Cardiogenic shockMI Killips IV
Hypotension[Palpatory 50]
Dopamine drip;Dopamine 4amps +250 D5W to run for 4mcg/kg/min
Levophed drip:
Levophed 4mg/ml +250cc D5w to run at2mg/kg/min
8/3/2019 patho ilben
http://slidepdf.com/reader/full/patho-ilben 3/5
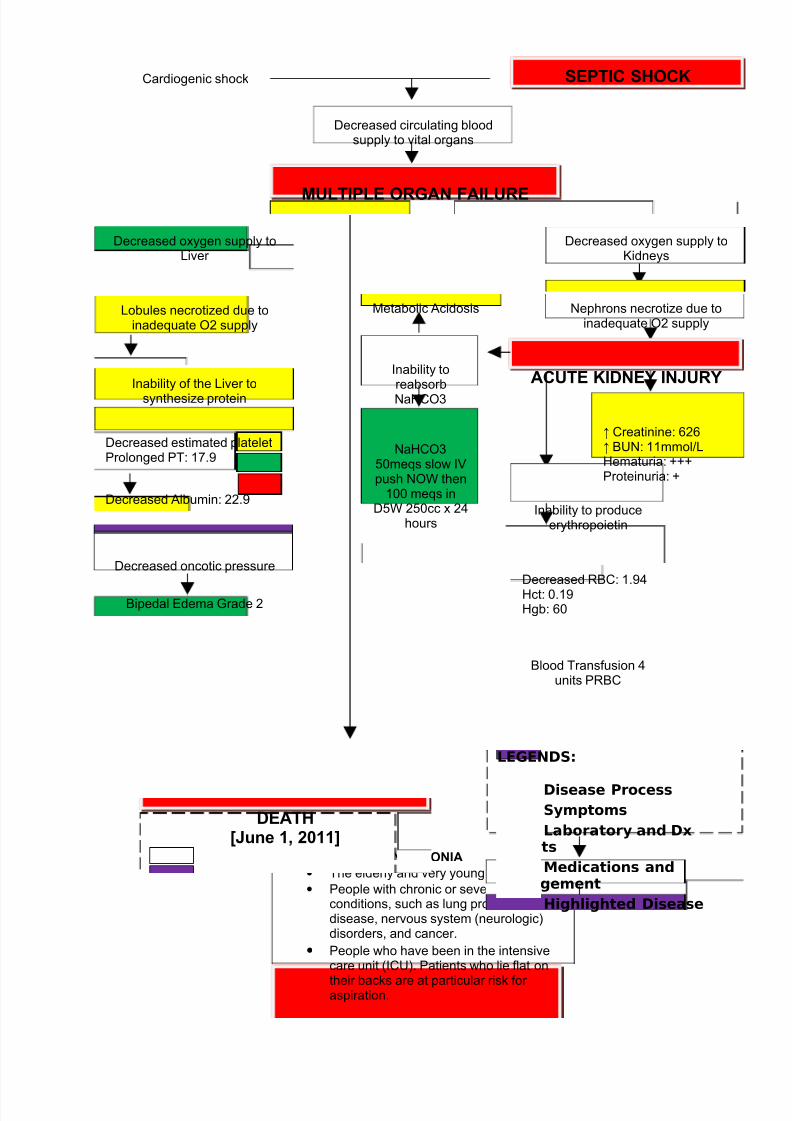
Cardiogenic shock
Decreased circulating bloodsupply to vital organs
MULTIPLE ORGAN FAILURE
Risk Factors for PNEUMONIA
• The elderly and very young.
• People with chronic or severe medicalconditions, such as lung problems, heartdisease, nervous system (neurologic)disorders, and cancer.
• People who have been in the intensivecare unit (ICU). Patients who lie flat on
their backs are at particular risk for aspiration.
SEPTIC SHOCK
Decreased oxygen supply toKidneys
Decreased oxygen supply toLiver
Lobules necrotized due toinadequate O2 supply
Nephrons necrotize due toinadequate O2 supply
ACUTE KIDNEY INJURY
↑ Creatinine: 626↑ BUN: 11mmol/LHematuria: +++Proteinuria: +
Inability to produceerythropoietin
Decreased RBC: 1.94Hct: 0.19Hgb: 60
Blood Transfusion 4units PRBC
Inability of the Liver tosynthesize protein
Decreased estimated plateletProlonged PT: 17.9
Decreased Albumin: 22.9
Decreased oncotic pressure
Bipedal Edema Grade 2
Inability toreabsorbNaHCO3
NaHCO350meqs slow IVpush NOW then
100 meqs inD5W 250cc x 24
hours
Metabolic Acidosis
DEATH[June 1, 2011]
LEGENDS:
Disease Process
Symptoms
Laboratory and DxResults
Medications andManagement
Highlighted Disease
8/3/2019 patho ilben
http://slidepdf.com/reader/full/patho-ilben 4/5
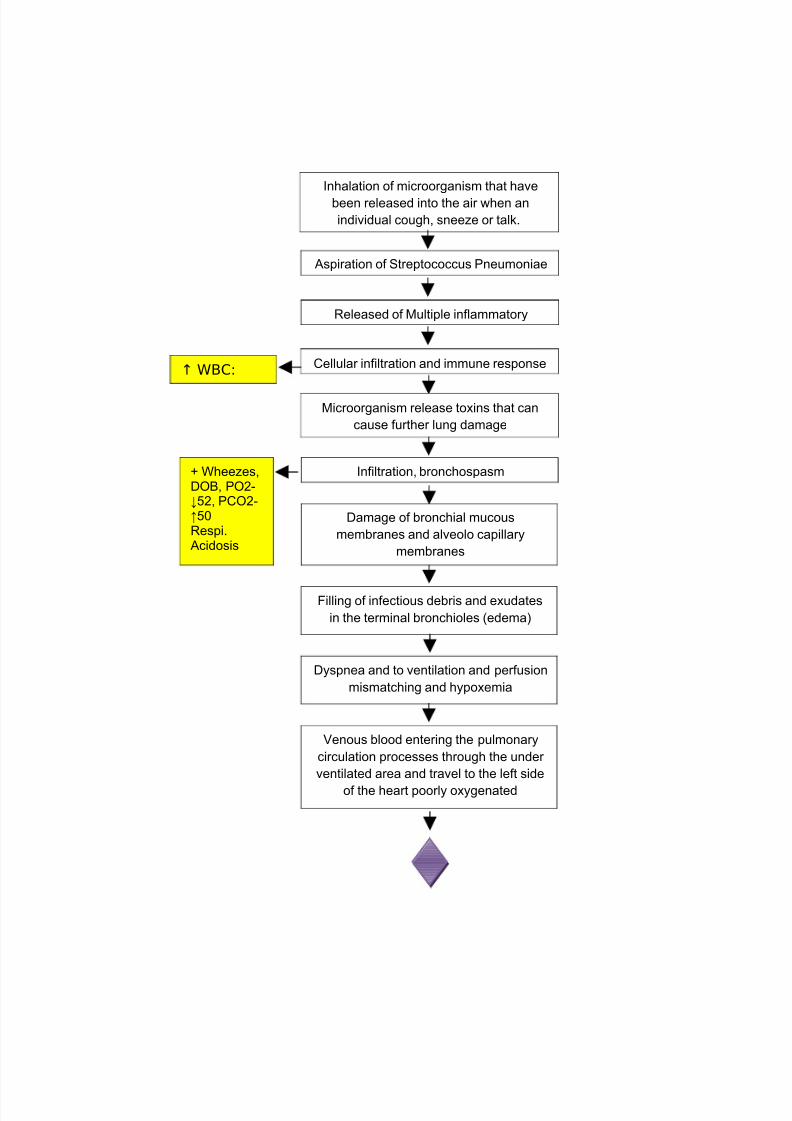
Inhalation of microorganism that have
been released into the air when an
individual cough, sneeze or talk.
Aspiration of Streptococcus Pneumoniae
Released of Multiple inflammatory
Cellular infiltration and immune response↑ WBC:
Microorganism release toxins that can
cause further lung damage
Infiltration, bronchospasm
Damage of bronchial mucous
membranes and alveolo capillary
membranes
Filling of infectious debris and exudates
in the terminal bronchioles (edema)
Dyspnea and to ventilation and perfusion
mismatching and hypoxemia
+ Wheezes,DOB, PO2-↓52, PCO2-↑50Respi.Acidosis
Venous blood entering the pulmonary
circulation processes through the under
ventilated area and travel to the left side
of the heart poorly oxygenated
8/3/2019 patho ilben
http://slidepdf.com/reader/full/patho-ilben 5/5
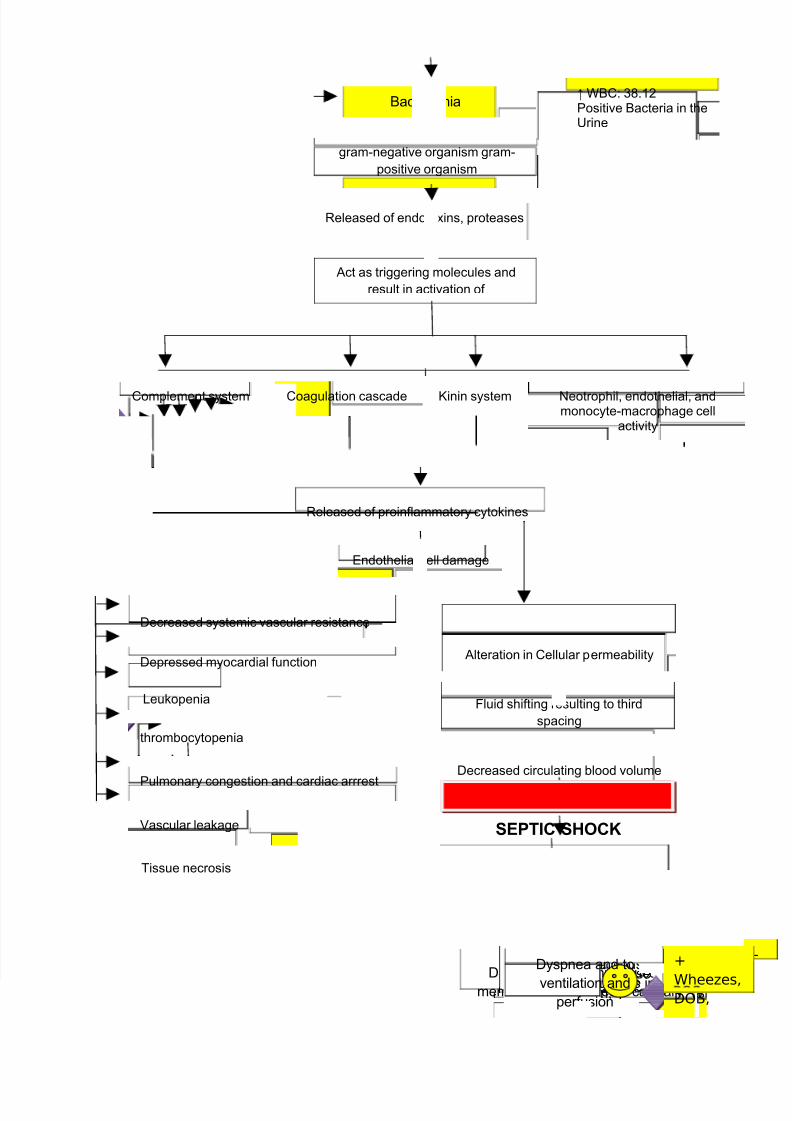
Pulmonary congestion and cardiac arrrest
Bacteremia
gram-negative organism gram-
positive organism
Released of endotoxins, proteases
Act as triggering molecules and
result in activation of
Neotrophil, endothelial, andmonocyte-macrophage cell
activity
Kinin systemCoagulation cascadeComplement system
Released of proinflammatory cytokines
Endothelial cell damage
Decreased systemic vascular resistance
Depressed myocardial function
Leukopenia
Tissue necrosis
Vascular leakage
thrombocytopenia
O2 Sa
70%
PO2-
Cellular infiltrationand immune
↑ WBC-
Microorganism release
toxins that can causeInfiltration,
Damage of bronchial mucous
membranes and alveolo capillary
Filling of infectious
debris and exudates inthe terminal
+
Wheezes,DOB,
Dyspnea and to
ventilation andperfusion
Alteration in Cellular permeability
Fluid shifting resulting to third
spacing
Decreased circulating blood volume
SEPTIC SHOCK
↑ WBC: 38.12Positive Bacteria in theUrine